An announcement of significance is coming.
Craig Childress, Psy.D.
Clinical Psychologist, PSY 18857

A Scientifically Based Model of "Parental Alienation"
We are going to establish a standard of practice in the assessment of attachment-related pathology surrounding divorce.
We are then going to move toward professional expertise. Mental health professionals who know what they’re doing – within standard and established constructs and principles.
Assessment leads to diagnosis, and diagnosis guides treatment.
It begins with assessment.
Attachment-related pathology is always created by pathogenic parenting. A child’s rejection of a parent (attachment-related pathology) is either being caused by the pathogenic parenting of the targeted-rejected parent (through hostile-aggressive child abuse), or it is being caused by the pathogenic parenting of the allied and supposedly “favored” parent (through the formation of a cross-generational coalition with the child against the other spouse-and-parent).
A semi-structured six-session treatment-focused assessment protocol can identify  the source of pathogenic parenting creating the attachment-related pathology.
the source of pathogenic parenting creating the attachment-related pathology.
The Assessment of Attachment-Related Pathology Surrounding Divorce
There are four mental health professionals that I know of who are qualified to conduct a treatment-focused assessment of attachment related pathology surrounding divorce. Each of these mental health professionals has trained with me personally, and each has direct access to me for consultation as needed. These four mental health professionals are Certified in AB-PA, including administration and documentation of the six-session treatment-focused assessment protocol.
We are establishing a ground foundation of professional knowledge in the standard and established constructs and principles of professional psychology required for professional competence, and ultimately for professional expertise.
The Attachment System
Family Systems Therapy
Personality Disorder Pathology
Complex Trauma
Does a mental health professional need to be “certified” to conduct a treatment-focused assessment protocol? No. Absolutely not. All mental health professionals should be conducting a treatment-focused assessment of attachment-related pathology surrounding divorce right now. It’s all standard and established professional psychology.
Can they? I have no idea. I am appalled by the degree of professional ignorance and incompetence that’s out there.
I do know this. There are four mental health professionals who can. They are the certified mental health professionals I worked with across three days of seminars in November. There are four mental health professionals who absolutely know how to conduct a treatment-focused assessment of attachment-related pathology surrounding divorce.
They have the knowledge, and they have my ear if they want consultation on a particularly troubling case. What’s more they have each other. They don’t realize this yet, but as things develop I’m planning to encourage a network of inter-professional consultation across AB-PA Certified mental health professionals; to use each other as resources of professional consultation.
What the Bowlby-Minuchin-Beck model of AB-PA provides is a shared common knowledge and language of professional psychology – cross-generational coalitions, emotional cutoffs, personality pathology, splitting, attachment trauma – all understood even before the consultation begins. The constructs of established professional psychology (Bowlby, Bowen, Beck, Minuchin, Millon) can unravel the diagnostic complexities and treatment issues.
There are four mental health professionals who are certified in AB-PA, who understand the pathology, who know what to do, and who are part of a growing network of professional collaboration.
They are not advocates or friends on Facebook; they don’t offer “advice” on what parents should do. They work with clients. They bring solution to family pathology for their clients. They are a verified source of high-level professional knowledge regarding attachment-related pathology surrounding divorce for families and the Courts. These four mental health professionals are:
Jayna Haney, MS, LPC Intern: Houston, Texas.
Advanced Certified in AB-PA
Ms. Haney is in a leadership role in bringing professional knowledge and expertise to the solution for “parental alienation.” She has studied with Karen Woodall in Great Britain as well as becoming Advanced Certified in AB-PA with me in November. Of additional note, Jayna is also trained in EMDR treatment for trauma and brings this additional trauma expertise to her work with the complex trauma of “parental alienation.” Jayna Haney has my full support, and she has my ear.
Jayna Haney: jayna@thebridgeacross.com
Michelle Jones, LCSW: Provo, Utah.
Advanced Certified in AB-PA
Michelle Jones, LCSW is a licensed clinical social worker who works with Concordia Families agency in Provo, Utah. Ms. Jones brings her AB-PA Advanced Certification into a professional clinic already experienced with the family pathology of “parental alienation” and court-involved families. Michelle Jones and the therapeutic team at Concordia Families has my full support, and they have my ear.
Michelle Jones: mjones@concordiafamilies.com
Concordia Families Website
Nadine Colgan, MS, NCC, LPCMH: Kennett Square, PA
Advanced Certified in AB-PA
Ms. Colgan brings a wealth of experience to her work. She holds a Master’s Degree in Counseling and Human Relations, she is a Licensed Professional Mental Health Counselor, she is a National Board Certified Counselor and a Certified Mediator. Ms. Colgan has extensive experience working with high-conflict divorce and is a strong resource in the Philadelphia, Wilmington, and Baltimore area.
Nadine Colgan: nadinecr1@nadinecolgan.com
Nadine Colgan Website
Larken J. Sutherland MS, LPC: Corpus Christi, Texas
Larken Sutherland is a Licensed Professional Counselor and Parenting Coordinator/Facilitator in private practice in Corpus Christi, Texas. Ms. Sutherland is experienced in working with high conflict families and she is Certified in AB-PA, she is a strong resource for families in the Corpus Christi area. Ms. Sutherland has my full support, and she has my ear.
Three others also received Certification in AB-PA, one is a legal professional, and two are parent-advocates.
JulieAnne Leonard
Advanced Certified in AB-PA
JulieAnne Leonard is an attorney who is completing her psychology degree in developmental psychology. Of note is that developmental psychology is a particularly useful domain of knowledge for understanding the influence of parenting on child development. Ms. Leonard has an extensive background serving as a Guardian ad Litem with high-conflict families. Through her legal background as an attorney, her extensive experience as a GAL, and her AB-PA Certification, Ms. Leonard represents an exceptionally strong resource for the Court in assisting the Court to identify “parental alienation” pathology and in coordinating effective treatment services for the family.
Peter Knudsen
Advanced Certified in AB-PA
Peter Knudsen is a parent-advocate located in the Netherlands. He is active in bringing the knowledge and protocols of AB-PA to the European mental health system and family courts. Peter and I are currently collaborating on several avenues for expanding AB-PA into the European mental health and family law systems. Peter has my full support and he has my ear.
Bryan Hale
Advanced Certified in AB-PA
Bryan Hale is a theology student and parent-advocate completing his degree in theology with the goal of becoming an ordained minister. I suspect the universe has designs for the life of Mr. Hale. He brings a unique array of talents to the solution, including a strong background in business and in creating organization support structures for projects and endeavors. Bryan Hale has my full support, and he has my ear.
Jayna Haney
Michelle Jones (Concordia)
Nadine Colgan
Larken Sutherland
I know that these four mental health professionals can conduct a treatment-focused assessment of attachment-related pathology surrounding divorce. These four mental health professionals are a verified resource for knowledge and professional skill sets for families, family law attorneys, and the Court.
As an attorney and Guardian ad Litem, JulieAnne Leonard also represents a strong resource for the Court in helping the Court to identify “parental alienation” and in coordinating the treatment.
Peter Knudsen, Bryan Hale, and I will be working behind the scenes on creating the support structures for change across the entire mental health and family court systems, for all children, everywhere.
As importantly… they are the core for a network of consultation support for each other, each bringing a different facet of knowledge, yet all with a common foundation of knowledge.
This is not about me. This is about you. You are the change. I am merely a catalyst. I am simply the clarion call returning professional psychology to the ground foundations of professional psychology; Bowlby, Minuchin, Beck, Millon, Bowen. You are the agents of change.
We are establishing a ground foundation of knowledge and standards of practice for the assessment, diagnosis, and treatment of attachment-related family pathology surrounding divorce. From this foundation, we then build professional expertise.
The ground foundation is not me. It’s Bowlby-Minuchin-Beck and the established constructs and principles of professional psychology.
This is about you and your children. This is about solving the family pathology of “parental alienation” for all children everywhere.
Craig Childress, Psy.D.
Clinical Psychologist, PSY 18857
I just wrote the following email to an attorney who was seeking consultation. I thought the information I provide might be more broadly of interest
To an attorney:
A child rejecting a parent is an attachment-related pathology. The attachment system is the brain system governing all aspects of love and bonding throughout the lifespan. A child rejecting a parent is a problem in the love and bonding system of the brain; in the attachment system.
The attachment system NEVER spontaneously dysfunctions. It ONLY becomes dysfunctional in response to pathogenic parenting (patho=pathology; genic=genesis, creation). Pathogenic parenting is the creation of significant pathology in the child through aberrant and distorted parenting practices.
Attachment-related pathology is always caused by pathogenic parenting, either from the mother or from the father. The diagnostic question is which parent is the source of the pathogenic parenting creating the child’s attachment-related pathology (the rejection of a parent). In this case, is it the mother’s parenting (child abuse), or is it the father’s parenting (a “cross-generational coalition” with the child against the targeted parent)?
Pathogenic parenting is an established construct in both clinical psychology and developmental psychology and it is used most commonly in reference to attachment-related pathology because the attachment system never spontaneously dysfunctions, but ONLY becomes dysfunctional in response to pathogenic parenting.
A “cross-generational coalition” is also a defined, standard, and established construct in family systems therapy.
The process of diagnosis regarding the source of pathogenic parenting is to evaluate the parenting practices of both parents.
We start with the parenting practices of the targeted-rejected parent. We assess the parenting practices of the targeted-rejected parent using:
The Parenting Practices Rating Scale
The Parenting Practices Rating Scale documents the findings from the assessment of the targeted parent’s parenting practices.
First, identify the category of parenting,
Abusive (level 1)
Severely Problematic (level 2)
Problematic (level 3)
Healthy (level 4)
Levels 1 and 2 parenting by the targeted-rejected parent would represent pathogenic parenting by this parent. Treatment for Levels 1 and 2 parenting should focus on changing the parenting behavior of the targeted-rejected parent.
Levels 3 and 4 parenting represent broadly normal-range parenting and could not account for a suppression in the child’s attachment bonding motivations toward a parent.
Next, rate the parenting of the targeted-rejected parent on a continuum from 0 to 100, from neglectful-uninvolved parenting (0) to hostile over-controlling parenting (100).
Normal range parenting is anything in the 25-75 range. Our preference in professional psychology is in the range of 40-60, but respect should be given to parents to define family values within their families and with their children, consistent with their personal, cultural, and religious values. Some parents will tend to be more permissive and lax, but still within normal-range expectations (ratings in the 30s), some parents will tend to be more firm, structured, and rule-oriented, but still normal-range (ratings in the 60s).
If a clinical assessment by the involved mental health professional identifies that the parenting practices of the targeted-rejected parent are in the normal range (documented as Category 3 or 4; and between 25-75 on the Permissive-to-Structured continuum), then the parenting practices of this parent are broadly normal-range and cannot account for the attachment-related pathology being evidenced by the child (a rejection of a normal-range attachment bond to the parent).
The next step is to assess the possibility of pathogenic parenting by the allied and supposedly “favored” parent. This becomes a little more challenging because the allied parent is hiding their negative-controlling influence on the child behind the child:
Allied Parent: “It’s not me, it’s the child who is refusing. I tell the child to go, but what can I do? I can’t force the child to go.”
The way to assess the pathogenic parenting of the allied parent is to lift the evidence of parental psychological control of the child from off of the child’s symptom features (the “psychological fingerprints” of parental control of the child).
We cannot psychologically control a child without leaving “psychological fingerprint” evidence of the control in the child’s symptom display.
Three symptoms in the child’s symptom display represent definitive diagnostic indicators of psychological control of the child by an allied narcissistic/(borderline) personality parent:
1. Attachment System Suppression: The suppression of the child’s attachment bonding motivations toward a normal-range parent.
2. Personality Disorder Traits: Five specific narcissistic personality traits in the child’s symptom display (grandiose judging of the targeted parent; absence of empathy toward the targeted parent; entitled expectations relative to the targeted parent; haughty and arrogant attitude toward the targeted parent; splitting/polarization of perception).
3. Persecutory Delusion: The child displays a fixed and false belief (a delusion) in the child’s supposed “victimization” by the normal-range parenting of the targeted parent (an encapsulated persecutory delusion).
When all three of these symptom indicators are present in the child’s symptom presentation – no other pathology in all of mental health will create this specific set of symptoms other than a cross-generational coalition of the child with a narcissistic/(borderline) parent against the targeted parent.
The presence of these three symptoms are documented using:
The Diagnostic Checklist for Pathogenic Parenting
If the involved mental health professional completes these two assessment documentation instruments, then I can absolutely tell you what the origins are for the attachment-related pathology in the family based on the symptom features displayed.
Normal-range parenting by the targeted parent and the three diagnostic indicators of pathogenic parenting by the allied parent are evident in the child’s symptom display… the pathogenic parenting creating the child’s attachment-related pathology is emanating from the allied and supposedly “favored” parent (a cross-generational coalition with the child against the other parent).
These two domains (potential pathogenic parenting by the targeted-rejected parent, and potential pathogenic parenting by the allied parent) can be assessed in six to eight treatment-focused assessment sessions.
I describe this six-session assessment protocol in the booklet:
The Assessment of Attachment-Related Pathology Surrounding Divorce
Pathogenic parenting that is creating significant developmental pathology in the child (diagnostic indicator 1), personality disorder pathology in the child (diagnostic indicator 2), and delusional-psychiatric pathology in the child (diagnostic indicator 3) represents a DSM-5 diagnosis of V995.51 Child Psychological Abuse, Confirmed.
Assessment leads to diagnosis, and diagnosis guides treatment:
In all cases of child abuse, physical child abuse, sexual child abuse, and psychological child abuse, the standard of practice and “duty to protect” requires the child’s protective separation from the abusive parent.
The child is then treated for the consequences of the child abuse, and the child’s healthy and normal-range development is recovered and restored.
Once the child’s healthy development is restored, the child’s relationship with the formerly abusive parent is then reestablished with sufficient safeguards to ensure that the child abuse does not resume once contact with the formerly abusive parent is reestablished. Typically, the abusive parent is required to obtain collateral individual therapy to gain and demonstrate insight into the prior abusive behavior (in this case, the psychological abuse of the child), and the level of safeguards for the child are typically based on the degree of cooperation and insight shown by the formerly abusive parent.
It is the confirmed DSM-5 diagnosis of V995.51 Child Psychological Abuse (based on the treatment-focused assessment using the Parenting Practices Rating Scale and the Diagnostic Checklist for Pathogenic Parenting) that serves as the professional and legal rationale for the protective separation period.
My typical recommendation is for a 9-month protective separation period.
An alternative to a protective separation period is available from a Strategic family systems intervention of a Contingent Visitation Schedule
Strategic family systems therapy (principle theorist: Jay Haley) is one of the two primary models for family therapy, the other being Structural family therapy (principle theorist: Salvador Minuchin). Strategic family systems therapy alters how the symptom confers power within the family.
A Contingent Visitation Schedule makes time with the allied pathogenic parent contingent upon the child remaining symptom free.
Custody is ordered as 50-50%. If the child develops symptoms (as determined by daily rating scales, monitored by the family therapist), then time with the allied pathogenic parent is reduced (to reduce the negative pathogenic influence of this parent who is creating the child’s symptoms), and time with the targeted parent is increased (to increase the time needed to repair the relationship being damaged by the pathogenic parenting of the other parent).
This increase-decrease time in visitation is defined within the structure of the Contingent Visitation Schedule. Once the child returns to non-symptomatic, custody visitation is returned to the shared 50-50% order.
The Contingent Visitation Schedule can be used prior to a protective separation, to give the allied parent one last chance to release the child from the coalition and allow the child to love both parents, or it can be used following the protective separation to ensure that the child psychological abuse does not resume once the distorted parenting of the allied pathogenic parent is reintroduced.
Summary
Parenting Practices Rating Scale
Diagnostic Checklist for Pathogenic Parenting
Assessment of Attachment-Related Pathology Surrounding Divorce
Contingent Visitation Schedule
Craig Childress, Psy.D.
Clinical Psychologist, PSY 18857
Definition of Cross-Generational Coalition
Jay Haley (1977)
“The people responding to each other in the triangle are not peers, but one of them is of a different generation from the other two… In the process of their interaction together, the person of one generation forms a coalition with the person of the other generation against his peer. By ‘coalition’ is meant a process of joint action which is against the third person… The coalition between the two persons is denied. That is, there is certain behavior which indicates a coalition which, when it is queried, will be denied as a coalition… In essence, the perverse triangle is one in which the separation of generations is breached in a covert way. When this occurs as a repetitive pattern, the system will be pathological.” (p. 37)
Haley, J. (1977). Toward a theory of pathological systems. In P. Watzlawick & J. Weakland (Eds.), The interactional view (pp. 31-48). New York: Norton.
Professional psychology is failing the family courts.
A child’s rejection of a parent surrounding divorce is a family therapy issue, not a child custody issue.
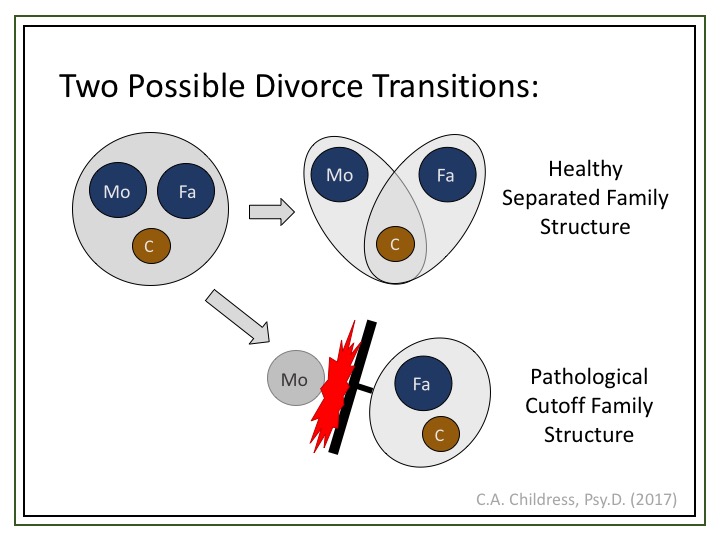
 The family’s successful transition to a healthy and functional separated family structure following divorce is always in the child’s best interests.
The family’s successful transition to a healthy and functional separated family structure following divorce is always in the child’s best interests.
Divorce ends the marriage, not the family. A cutoff family structure is always pathological. A cutoff family structure is NEVER a healthy post-divorce family.
 It is always in the child’s best interests for the family to transition to a healthy and functional separated family structure following divorce.
It is always in the child’s best interests for the family to transition to a healthy and functional separated family structure following divorce.
The courtroom is not the proper venue to solve family pathology. Family pathology cannot be litigated. The resolution of family pathology is the domain of professional psychology.
The legal system therefore turns to professional psychology for consultation on family pathology.
This request for consultation takes one of two forms, an order for something called “reunification therapy” or an order for a child custody evaluation by professional psychology.
In each of these, professional psychology is failing the court.
First, there is no such thing as reunification therapy. This is important to understand. There is no such thing as reunification therapy. It’s an entirely made up thing. There is no book, no article, no theorist who has ever described anything called “reunification therapy.” It’s a sham construct designed to allow the “reunification therapist” to just make stuff up and do whatever they want, and just call it “reunification therapy.”
I’m a clinical psychology. Psychotherapy is what I do, and I don’t think I’m being clear enough about this yet:
“Reunification therapy” is a snake-oil remedy of unknown contents that is more likely as not to kill you as to cure ya. If any mental health person says they do “reunification therapy” – run. There is no such thing as “reunification therapy.”
There, is that clear enough?
If any mental health professional disagrees, there is a Comment section to this blog. Cite for me a single book or article that describes what “reunification therapy” is.
Crickets. Nothing.
What the court and all parents want is family systems therapy; either Structural family systems (Minuchin) or Strategic family systems (Haley; Madanes). Bowen has a foundational family systems model (Bowenian family systems therapy; The Bowen Center). Satir has a model strong on family communication dynamics.
A competent family systems therapist is knowledgeable about all of these variations. They all center around the same basic core constructs of Bowen; elaborated by Munichin and Haley.
Family systems therapy is one of the four primary schools of psychotherapy, the others are psychoanalytic psychotherapy (think Freud and his couch), cognitive-behavioral therapy (think lab rats pressing a lever), and humanistic-existential psychotherapy (think hot tub in Esalen).
Family systems therapy is the only school of psychotherapy that is designed to address and solve current family relationship conflict. Family systems therapy is the appropriate form of psychotherapy for addressing and resolving family-related conflict surrounding divorce.
The pathology of a child-rejecting a parent surrounding divorce is called an “emotional cutoff” (Bowen). This is not Dr. Childress saying this. This is Murray Bowen saying this. Standard family systems construct.
The pathology of an “emotional cutoff” is caused by disturbances in the process of “differentiation” within and among the family members. Read:
Bowen Center: Eight Concepts
2. Differentiation of Self
This is not Dr. Childress. This is Bowen. Standard family systems therapy. Disturbances in differentiation within family members can lead to the child’s “triangulation” into the spousal conflict to stabilize a parent’s vulnerability.
The child’s “triangulation” into the spousal conflict can take the form of a “cross-generational coalition” with one parent against the other parent, resulting in an “emotional cutoff” in the child’s relationship with the targeted parent.
Triangulation
Cross-generational coalition
Emotional cutoff
Differentiation of self
All standard family systems therapy stuff. Bowen, Minuchin, Haley.
There is no such thing as “reunification therapy.” No book. No article. No theorist. The court and parents want family systems therapy.
Structural family systems therapy (Minuchin)
Strategic family systems therapy (Haley, Madanes)
Bowenian family systems therapy (Bowen)
Problem 1: Professional psychology is failing to provide the court with the proper professional knowledge and expertise needed to solve attachment-related family pathology surrounding divorce. Instead, mental health persons surrounding the legal system are simply making stuff up willy nilly.
Problem 2: Child custody evaluations.
This is important to understand: There is no scientifically established support for the validity of child custody evaluations.
Child custody evaluations violate every standard of professional practice regarding the development of an assessment procedure. I discuss all of this more fully in:
The Child Custody Industry in Mental Health
There are multiple-multiple devastating problems with the practice of child custody evaluations, but I’ll focus here on just one, the most devastating one: No inter-rater reliability.
The conclusions and recommendations reached by child custody evaluations have no inter-rater reliability. What this sentence means is that two different evaluators can reach two entirely different sets of conclusions and recommendations based on exactly the same data.
Well, that’s a problem. According to the axioms of assessment, if an assessment procedure is not reliable (does not produce stable results), then the assessment procedure CANNOT – by definition – be valid. The conclusions and recommendations from child custody evaluations are not valid.
If there is no inter-rater reliability, the conclusions and recommendations of child custody evaluations are simply the opinions of one person, that specific evaluator, perhaps based loosely on some psychological principles, perhaps based on no psychological principles whatsoever, just a matter of the individual opinion of the evaluator.
Don’t believe me? There is a Comment section to this blog. I challenge any mental health professional to cite for me a single study indicating the inter-rater reliability of the conclusions and recommendations reached by child custody evaluations.
Crickets. Nothing.
The conclusions and recommendations of child custody evaluations are no more valid than a monkey throwing darts at a dart board, and a lot less entertaining – and, I might add, far more expensive. Child custody evaluations are a very lucrative industry for professional psychology surrounding the family courts.
Child custody evaluations are a financial racket, pure and simple. That is a strong professional statement to make, and I am absolutely prepared to back it up anytime, anywhere. If any mental health professional wants to take exception to my statement, cite for me a single study identifying the inter-rater reliability of child custody evaluations. If an assessment procedure is not reliable, it cannot, by axiomatic definition within professional assessment, be valid. Child custody evaluations are a financial racket, pure and simple:
Do child custody evaluations actually do anything to solve the family pathology? No. Of course not. They’re “evaluations” – not “therapy.” For therapy, you’ll need “reunification therapy.”
 See, right here in Recommendation 3 of the child custody evaluation, right after Recommendation 2 that custody time-share should remain exactly where it is right now (with the child rejecting one parent), see, a recommendation for “reunification therapy.”
See, right here in Recommendation 3 of the child custody evaluation, right after Recommendation 2 that custody time-share should remain exactly where it is right now (with the child rejecting one parent), see, a recommendation for “reunification therapy.”
Child custody evaluations don’t actually fix things, they just tell the court to keep things where they are right now (with the child rejecting one parent) and do “reunification therapy.”
And do you know what the “reunification therapist” is going to say?
“We need to go slowly and not rush the child. We’ll start with 2 hours of supervised visitation and then increase it from there as the child decides they want to spend time with the parent. We don’t actually want to solve the family pathology of a cutoff family relationship.”
“We need to go “slowly” – a consistent hour of “therapy” on my schedule every week. Court-ordered, month after month, year after year. But nothing actually changes, because “reunification therapy” isn’t really a form of therapy. It’s just designed to give pablum to the court as if something was taking place.”
But the child never “decides” to spend more time with the targeted parent. Surprise, surprise. In fact, things get worse, and worse, and worse, throughout all of the “reunification therapy.”
It is the responsibility of professional psychology to treat and resolve family pathology. That’s our job.
Professional psychology is failing the family court system. Professional psychology is not providing the court with the proper professional expertise required to solve the family conflict.
The court and parents don’t want or need a pointless child custody evaluation. If you’re tempted to conduct a child custody evaluation I suggest you hire a monkey with darts instead; it’ll be more entertaining and equally as valid.
The court and parents don’t want a mythical “reunification therapy,” a snake-oil therapy that solves nothing, ever.
The court and parents want family systems therapy – real psychotherapy that will solve the family conflict and facilitate the family’s successful transition to a healthy and functional separated family structure following divorce, which is always in the child’s best interests.
It is time for professional competence based in the standard and established constructs and principles of professional psychology.
Family systems therapy: Bowen, Minuchin, Haley.
The finger that points at the moon is not the moon.
Craig Childress, Psy.D.
Clinical Psychologist, PSY 18857
A question was posed to me. I thought my answer might be of broader interest.
There are five answers to this question
In attachment-based parental alienation (AB-PA), there are three diagnostic indicators, and the identification of AB-PA is made based on all three being present.
Attachment System Suppression: A child’s rejection of a normal-range and affectionally available parent.
Personality Disorder Traits: Five specific narcissistic personality traits displayed by the child.
Persecutory Delusion: The child evidences a fixed and false belief (a delusion) in the child’s supposed “victimization by the normal-range parenting of the targeted-rejected parent.
All three of these symptoms must be present.
Answer 1 to the question “Is rejection of a parent a problem for the child?” is that the creation of significant developmental pathology (diagnostic indicator 1), personality disorder pathology (diagnostic indicator 2), and delusional-psychiatric pathology (diagnostic indicator 3) in the child is damaging to the child’s healthy psychological development.
Creating significant psychopathology in the child is damaging to the child.
This is a sufficient answer, but there are 4 more equally sufficient answers.
The second answer to this question is to recognize the importance of each type of parent-child relationship to the child’s healthy development. There are four types of parent-child relationships:
Mother-son
Father-son
Mother-daughter
Father-daughter
Each of these relationships is unique. None are interchangeable. None are expendable.
I discuss this on pages 1 and 2 of the Assessment of Attachment-Related Pathology Surrounding Divorce:
“Families contain four primary types of parent-child relationship; mother-son, mother-daughter, father-son, father-daughter. The benefits to the child from each of these relationship types is unique to that relationship, they are not replaceable or interchangeable in the value they provide to the child because each confers unique and vital developmental experiences that are immensely important for the child’s healthy emotional and psychological development.
Mother-son bond: The deep emotional and psychological connection between a male child and his mother is potentially one of the most affectionate parent-child bonding types. A positive and healthy mother-son bond creates for the child a deep inner sense of the child’s inherent value as a person, and the mother-son bond forms the basis for the child’s emotional security. The quality of the mother-son bond also establishes the template of expectations (the “internal working models”) for the later formation of the child’s spousal relationship in marriage.
Mother-daughter bond: The mother-daughter bond can be one of the most complex parent-child relationships as the mother psychologically re-experiences herself and her own childhood in her daughter’s development. The daughter draws important self-worth and gender identity modeling from a positive and healthy mother-daughter bond, and the mother-daughter bond serves as the template for the daughter’s future role as a mother for her own children. Daughters become future mothers, and the relationship template formed in the mother-daughter bond carries important implications for the daughter’s future parenting with her own children.
Father-son bond: The son’s emotional and psychological bond with the father provides essential self-esteem and gender identity modeling for the child. The son’s healthy emotional and psychological bond to his father provides important communications of support from the father for the male child’s sense of self-value as an emerging young man, and the son’s bonded relationship with his father provides critical support for the child’s development of the maturity that leads to the child entering the world as an emotionally mature and responsible young man.
Father-daughter bond: A daughter’s relationship with her father is one of the most affectionally important of the parent-child relationships. The daughter develops the core foundation for her self-worth from her affectionally bonded relationship with her father (an affectional process exemplified by the classic family roles as “daddy’s princess” and “daddy’s little girl”). As a primary relationship pattern, the father-daughter relationship also serves as the template (the “internal working model”) that will guide the formation of her future spousal relationship with her own husband during marriage.
Each of these primary relationship types is unique, and the special value that each of these relationship types confer to the child is not interchangeable through the child’s relationship with the other parent. The mother-son relationship offers a special loving warmth and richness in the child’s development that is not interchangeable with the value offered to the son by the male-male affectional bond he has with his father. The father’s relationship with his daughter is similarly filled with deep warmth and enriching love, and it is not interchangeable with the rich complexity of the mother-daughter bond. The child benefits from each of these unique relationships within the family, and each relationship type merits the full support of both parents and the Court in nourishing its development…
Attempting to compare the relative benefits received by the child from any of these primary relationship types is an impossible task. The scientific and professional literature in developmental and clinical psychology does not allow for a comparison of parenting to determine the “better parent” that would warrant truncating the child’s opportunity to develop any of the entirely unique parent-child bonding relationships within the family. Each parent brings unique benefits from a complex relationship with the child that cannot be replaced or duplicated by the other parent. The unique developmental benefits that accrue from the son’s relationship with his father is not interchangeable with the unique emotional and psychological benefits found in the son’s bonded relationship with his mother. Similarly, the benefits to the daughter from an affectionally bonded relationship with her mother are unique to that relationship and are not interchangeable with the unique emotional and psychological benefits to the daughter acquired through her affectionate bond to her father. Each relationship type within the family – father-son; father-daughter; mother-son; mother-daughter – is unique, special, and critically important to the child’s healthy development.”
Childress, 2017; Assessment of Attachment-Related Pathology Surrounding Divorce, p. 1-2)
A child’s psychological identity is embedded in two families. The child’s self-identity is a combination of two heritages, one from the mother’s side of the family’s origins, and one from the father’s side of the family’s origins. A child’s self-identity formation is grounded within two families of origin.
A child’s rejection of one parent is the child’s rejection of one half of the child’s self-identity. The rejection of a foundational component to self-identity will significantly damage the child’s healthy development of identity structures.
While damage to self-identity development is of concern throughout childhood, this becomes a particularly preeminent concern during the child’s adolescent period of identity development. It is extremely valuable for the adolescent to have a healthy and bonded relationships with both parents, both halves of the child’s self-identity, during the identity development period of adolescence.
A child’s rejection of a parent is prominently damaging to the child’s development of self-identity.
Childhood is the time period for learning the skills needed in successful adulthood. Conflict resolution in intimate relationships is an essential adult life skill, vital to later healthy emotional and psychological functioning in adult relationships.
When conflict develops in intimate partner relations, it is important to know how to repair these ruptures in the relationship. Interpersonal conflict in family relationships happens all the time, it is important to know how to repair relationships, how to fix conflict. A “cutoff” family relationship (Bowen) is never healthy, it is always pathological. The ability to repair breaches to relationship is a key feature of healthy psychological functioning.
Allowing the child to remain in a breached relationship with a parent is never healthy, it is simply sustaining the pathology of trauma contained and being transmitted within the family. Healing involves the restoration of relationship bonds. Healing is always a good thing.
Children benefit immensely from parental love. For a child, parental love is the manna of life.
Children have the right to receive the love of both parents and from each parent, fully, richly, and in all of its wonderful complexity.
For a child, the love of a parent fosters an immensely powerful psychological bond of deep shared intimacy with the parent, with each parent, unique to their relationship. With each parent, and through both parents, the child develops a special and unique relationship of great importance to the child’s core sense of self-worth and core value.
From each parent, and through both parents, the child learns the lessons of life contained in the personal fabric and family of origin story for that parent, embedded within that parent’s ways of being. The life experience embedded in each parent helps form the substance of the child by informing the quality of their relationship. Life moves through generations.
Children have the right to be loved by each parent, and by both parents. And by grandmothers and grandfathers, by aunts and uncles and cousins, by family. And by friends, coaches, teachers, everyone. Love is good for a child, it is their manna of life.
When a parent wants to love a child, this should happen. It is immensely healthy for the child.
Children have the right to be loved by both parents.
Craig Childress, Psy.D.
Clinical Psychologist, PSY 18857
I have just mailed packages containing a cover letter, the Petition to the APA, and 350 pages of your signatures to the leadership of four organizations:
Jo Linder-Crow, PhD
Executive Director
California Psychological Association
1231 I Street, Suite 204
Sacramento, CA 95814
David White, CAE
Executive Director
Texas Psychological Association
7625 White Oak Drive
P.O. Box 1930
Cedar Park, TX 78630
Krista Paternostro
Executive Director
Pennsylvania Psychological Association
416 Forster Street
Harrisburg, PA 17102-1748
Nicola Gale
President, British Psychological Society
St Andrews House
48 Princess Rd E
Leicester LE1 7DR, UK
Your turn. Same organizations. 14,727 letters asking them to review and endorse the Petition to the APA.
It doesn’t matter where you are. It doesn’t matter if you live in a different state or different country, 14,728 voices directed toward four organizations. Don’t let me work harder for your children than you do. Work for each other, work for all children everywhere. And we’ll work for your children, each for the other. When you come together in a single voice, you are more powerful than you know.
Then, do you know what I’ll do next? I’ll select another four states and I’ll send each of them a cover letter, the Petition to the APA, and 350 pages of your signatures – or 400 pages, or 800 pages, whatever you give me to work with. I will take your voice to professional psychology. The strength of that voice is up to you.
I am going to continue selecting psychological organizations from the list:
Psychological Association Directory
There’s a reason I selected each of the first four.
California is obviously my home state.
Texas has developed a substantial foundation in creating the change. Dwilene Lindsey and Children4Tomorrow are a force to be reckoned with. I’m sure they could use your support. If you have any financial resources and you want to make a donation to end “parental alienation” and support healthy child development, Children4Tomorrow would be my strongest recommendation.
They will absolutely 100% put the money to good use protecting children from the psychological child abuse of “alienation” surrounding divorce.
Pennsylvania also has active forces moving for change, and through individual efforts were able to get me invited to present to their state legislature. I think I was successful in bringing your voice to them. Things are moving forward in Pennsylvania. There are other active states, Florida has psychological child abuse legislation submitted, New York, North Carolina, Arizona, and others are churning with activity.
I chose Great Britain because it is the home of John Bowlby and attachment theory. Honoring the authenticity of the attachment bond to both parents belongs in Great Britain. It is overdue for Great Britain to claim its leadership in solving attachment-related pathology.
Creating and mailing a submission packet of 350 pages of signatures costs me about $50 per packet, and I plan to send packets to the psychological associations of each of the 50 states and multiple foreign psychological associations. Why am I doing this? Why am I spending my money on your kids? Because your children need me to do it.
We are going to solve this for all children everywhere.
It would be much less expensive if I didn’t send 350 pages of your signatures. I’m sending 350 pages of your signatures.
As I was downloading your signatures, I scrolled through all 350 pages of signatures. Each name, each family, each bond of love – destroyed. It was emotionally powerful, to hear each voice speak on 350 pages. I’m sending 350 pages of your signatures because I want them to hear your voice as I hear your voice.
The pathology of “parental alienation” must end.
The time of battle for your children is now. We will no longer tolerate the destruction of children’s lives, we will no longer tolerate the destruction of families.
We will no longer tolerate the psychological abuse of children.
You are the warriors for your children, and the time of battle is now. We are on the battlefield now. We need your voice, now.
These submissions to professional organizations are not designed to have an effect on the organization, they’re designed to have an effect on you. Don’t let me fight harder for your children than you do. 14,729 voices directed toward four organizations. Make a statement to these four organizations.
And then we will select the next four.
I will do everything I can to take your voice to professional psychology, because your children need me to do that. This is a narcissistic pathogen. The solution is the opposite of narcissistic, it is empathy for the other, doing for the other. It must become about solving this for all children everywhere, not just for the children in this or that specific family.
No matter what state or nation you live in, work for each other. Come together into a single voice, an unstoppable voice for change.
Start with these four organizations. Be kind, always be kind. And be relentless. Then we will select the next four. We are going to solve this for all children everywhere. Because your children need us to.
Craig Childress, Psy.D.
Clinical Psychologist, PSY 18857

Dr. Bernet,
It’s come to my attention that you’re not aware of my offers to collaborate and work together. That’s unfortunate. That must mean that you’re not subscribed to my blog. That too, is unfortunate. Is that because you don’t think I have anything valuable to say?
To clarify, I offered collaboration in the blog post from September:
Dr. Bernet, join me. (posted 9/5/17)
Let me reiterate from my post in September;
From Dr. Bernet, join me (posted 9/5/17):
The diagnostic paradigm for the attachment-related pathology commonly called “parental alienation” is changing.
I’m asking for you to join me in creating this change.
You have been a stalwart and steady warrior for targeted parents through all of these years. I saw how you tried to influence the formation of the DSM diagnostic system… You have fought a heroic struggle against the pathology for many years. Admirable. Magnificent.
But ultimately, the Gardnerian PAS model has fatal flaws embedded within it. You didn’t have the proper tool to solve the pathology. I can tell you exactly what those inherent and terminal problems with the Gardnerian PAS model are – but not now.
The construct of meme-structures will help you understand a lot of things.
Gardnerian PAS is a failed diagnostic paradigm.
The only issue that is relevant at a professional-level is the solution. It is not relevant how many angels can dance on the head of a pin.
AB-PA provides a solution.
Gardnerian PAS does not.
The world is changing.
Stop fighting against AB-PA and fighting against the change it brings. I am not the source of this change, I am merely the conduit. There are larger forces at work here.
I would like to propose that we write two collaborative articles together, Dr. Bernet.
The first one would be a reflection on history and the future. It would pass the torch from Gardnerian PAS to AB-PA for the solution. We’re both a couple of old guys, Dr. Beret. This isn’t about us. There will be a new generation coming to take on the fight against the pathology.
AB-PA is a richer diagnostic model than the Gardnerian model because AB-PA opens wide the full data sets of attachment theory, intersubjectivity, personality disorder pathology, family systems therapy, and complex trauma.
The categorical AB-PA diagnostic framework lends itself better to “operationally defining” the construct of “parental alienation” for research purposes, and those 12 Associated Clinical Signs are jewels – both clinically and from a research perspective.
It will be impossible to prevent AB-PA from fully entering professional discussion and professional practice. Help me to define the legacy of our fight against the pathogen to the next generation.
I propose that in the first half of a joint collaborative article, you describe the first-fight against the pathogen. Tell us about Gardner’s courage, the malevolence of the pathology, all the research and the battle surrounding Gardnerian PAS. Bring out whatever data sets you want and revel in it.
And then end your segment of the article by passing the torch for the solution to AB-PA.
Then let me take the second half of the article to explain that, as courageous and magnificent as Gardner may have been, he skipped the step of diagnosis; the application of standard and established constructs and principles to a set of symptoms. Instead, he too quickly abandoned the rigors of professional practice by proposing a “new form of pathology” which led professional psychology away from the standards of professional practice regarding diagnosis; the application of standard and established constructs and principles to a set of symptoms (no “unique new forms of pathology” diagnostic proposals).
I’ll describe how AB-PA returns to the foundations of the pathology and corrects this diagnostic step skipped by Gardner. AB-PA defines the pathology (the set of symptoms) from entirely within standard and established constructs and principles. Here’s what AB-PA says; pathological mourning, the trans-generational transmission of attachment trauma, the addition of splitting pathology to a cross-generational coalition, we need to return to standard and established constructs and principles in our professional diagnosis of pathology, and AB-PA does this.
You and I, in a joint article, bring together both the history and the future of our efforts to solve the pathology of “parental alienation.”
Then, let’s write a second article together. A much more interesting article. Let’s set the stage for completing your work with the DSM diagnostic system. Let’s set the stage for the next generation in their efforts to include the pathology of “parental alienation” into the DSM diagnostic system.
Together, you and I in a joint article, let’s make the argument to the DSM that this pathology is an attachment-trauma pathology that belongs in the Trauma and Stressor-Related section of the DSM. In doing that, we then have a specific committee we’re targeting for support – we are forming allies within the DSM process – a new Trauma and Stressors disorder – attachment trauma – the trans-generational transmission of attachment trauma.
We will argue that the diagnosis should be nearly identical to the prior DSM-IV TR diagnosis of a Shared Psychotic Disorder. Nearly the same identical everything. Look how closely that DSM-IV diagnosis mirrors the pathology of “parental alienation”:
DSM IV TR Shared Psychotic Disorder
Diagnostic indicator 3 of AB-PA is the encapsulated persecutory delusion. What do you want to bet that we will find massive amounts of overlap in the psychological process that the Shared Psychotic Disorder people were looking at for the original DSM-IV disorder, and the pathology we’re looking at with AB-PA.
The DSM system has already acknowledged in the DSM-IV that the pathology of a shared delusion exists. They acknowledge it in DSM-5 but diagnostically bury it. All we’ll be asking for is that they re-establish the shared delusion – just like in the DSM-IV – as a primary diagnosis in the Trauma and Stressor-Related section, and we link our reasoning to the shared delusion created by the trans-generational transmission of attachment trauma.
We can bring all of the data sets from attachment theory, intersubjectivity, personality disorder pathology, and complex trauma to our argument.
You and I are old guys, Dr. Bernet. This DSM battle is for the next generation of mental health warriors. But you and I could lay out the vision for how that battle can be fought and won – the trans-generational transmission of attachment trauma creating a shared delusional disorder (Trauma and Stressor-Related section of the DSM – right alongside the other attachment-related disorders).
The world is changing, Dr. Bernet. There are larger forces at work in this. This isn’t Dr. Childress. I’m merely the conduit for catalyzing the change. The only credit to me is that I’m smart enough to recognize my role in what the universe wants to do. Join with me in creating this changed world. Trying to stop the change is like trying to hold back the ocean by putting up your hands to stop the waves from crashing on the shore.
Join me in defining the legacy and the future of our fight with the pathogen. Trust me, Gardner doesn’t care about his model, he just wants us to defeat the malignancy of this pathogen. Do you know what I think Gardner would say to me? “Go for it, Dr. C.” I am fully convinced that Gardner is supportive of my efforts with AB-PA. He doesn’t care about “his” model, he just wants us to defeat the pathogen and solve the pathology. He wants us to finish what he began, he wants us to defeat the pathogen.
But in the interesting way that the universe works, we will fulfill Gardner’s legacy without Gardner’s model. Curious, isn’t it. But it’s not surprising to me, because that’s the way things work sometimes.
We can fulfill his wishes using AB-PA. When we bring the full power of scientifically established data sets to the solution, we can solve the pathology for all children and all families everywhere.
Join us, Dr. Bernet. Join me. Let’s write two collaborative articles. One to reflect on history and the future, and one to define for future generations the path forward to achieve formal inclusion of the pathology into the DSM diagnostic system.
Craig Childress, Psy.D.
Clinical Psychologist, PSY 18857
From Dr. Bernet, join me. (posted 9/5/17)
I am asking you to formally endorse and actively support the Petition to the APA.
We are on the battlefield now. Today. We need your support. Targeted parents and their children need your support. Now. Today.
You are the professional organization representing targeted parents. You are the professional organization of support for them. It is to your role that advocacy for the Petition to the APA falls.
It is you who should be seeking formal endorsements to the Petition from professional psychology organizations and professional legal organizations worldwide.
The world is changing. The work of Bowlby and Minuchin and Beck is replacing the work of Gardner. We are returning to standard and established constructs and principles of professional psychology to define, diagnose, and treat pathology. Professional psychology will become united around the work of Bowlby and Minuchin and Beck, and the professional standards of practice that this brings.
In defining the pathology entirely within standard and established constructs and principles, the Bowlby-Minuchin-Beck model of attachment-based “parental alienation” (AB-PA) defines domains of knowledge needed for professional competence.
The attachment system
Personality disorder pathology
Family systems therapy
Complex trauma
All mental health professionals can unite around standard principles of professional psychology for basic competence. Targeted parents and their children need your voice. They need you to stand with them in their call for basic professional competence.
The 14,175 voices of the Petition are asking for yours; 14,179 voices are asking the PASG to formally endorse and actively support the Petition to the APA.
This is your purpose. To bring your united voice to solving “parental alienation” for all children everywhere.
To help targeted parents create the change they need to restore their families.
Join them. Join with the 14,181 voices in support of the Petition to the APA.
The battle to reclaim the American Psychological Association as an ally of targeted parents is here. The battle is now. We need your voice now.
The 14,183 voices of the Petition to the APA are asking you to formally endorse and actively support the Petition to the APA.
Craig Childress, Psy.D.
Clinical Psychologist, PSY 18857
Divorce ends the marriage. It does not end the family. When there is a child there will always be a family.
Divorce involves the transition of the family from an intact family structure united by the marital bond, to a separated family structure united by the parent-child bonds.
If you are a mental health professional working with a dysfunctional family transition from an intact family structure (united by the marriage) to a healthy separated family structure (united by the shared bonds of affection between the child and both parents), then understanding the process of family transitions is central to your professional responsibility.
The pathology of a child rejecting a parent surrounding divorce is called a “cutoff” family structure (Bowen).
If you are a mental health professional who doesn’t know what a cutoff family relationship is, you need to stop right now and learn about Murray Bowen and family systems therapy. Murray Bowen is one of the foundational figures in family systems therapy. His work provides a ground understanding for the processes in families, especially this type of dysfunctional family.
Once you have read and understand Bowen family systems, study specifically the construct of “emotional cutoff.” What people are calling “parental alienation” is an emotional cutoff in the parent-child relationship. It is essential to professional competence in assessing, diagnosing, and treating this type of family pathology, that all mental health professionals know and understand Murray Bowen’s construct of an emotional cutoff.
For all mental health professionals working with attachment-related pathology surrounding divorce, read Titelman.
Titelman, P. (2003). Emotional Cutoff: Bowen Family Systems Theory Perspectives. New York: Haworth Press.
“The origins of the concept of cutoff are rooted in Bowen’s parallel early understandings of differentiation, triangles, the nuclear family emotional process, family projection process, and multigenerational transmission process.” (Titelman, 2003, p. 16)
“Bowen theory postulates two main variables in human functioning: anxiety and differentiation. His theory makes the distinction between acute and chronic anxiety. Acute anxiety occurs in response to real threats and is time-limited. Chronic anxiety generally occurs in response to imagined threats and is not experienced as time-limited. Acute anxiety is fed by fear of what is: chronic anxiety is fed by fear of what might be (Kerr & Bowen, 1988, p. 113)” (Titelman, 2003, p. 20)
Bowen’s constructs of differentiation and emotional cutoff are centrally relevant to working with attachment-related pathology surrounding divorce. If you are a mental health professional working with attachment-related pathology surrounding divorce and you do not know Murray Bowen’s work on differentiation and the emotional cutoff, stop what your doing. Stop. Seriously, Stop. Learn about Murray Bowen and the constructs of differentiation and emotional cutoffs.
It’s a matter of basic professional competence. Bowen. Emotional cutoff.
A cutoff family structure after divorce is always pathological. There is no such thing as a “healthy cutoff family structure.”
A cutoff family structure is always a symptom of pathology in the family, having to do with psychological boundaries and differentiation within the family. Bowen.
It is vital that all mental health professionals working with attachment-related pathology surrounding divorce understand Bowen, particularly the construct of “emotional cutoff.”
This is standard foundational family systems therapy stuff. Bowen. Murray Bowen. Emotional cutoff.
There are four parent-child relationship types;
The mother-son relationship;
The father-son relationship;
The mother-daughter relationship;
The father-daughter relationship.
Each of these relationship types is unique. Each is essential to the healthy development of the child. None of these relationships are interchangeable. None of these relationships are expendable.
The value of each of these relationship types should receive the full support of professional psychology, and from the family courts.
It is ALWAYS in the child’s best interests to maintain a full and complex relationship with both parents. It is ALWAYS in the child’s best interest that the family make a successful transition following divorce from the previous intact family structure (united by the marriage) to a healthy separated family strucutre (united by the child, and by the child’s shared bonds of affection with both parents).
The mother-son bond can be a deeply emotional bond. Much of the son’s foundational self-worth is created in the mother-son bond. As the son matures into adulthood, the mother-son bond serves as the template for the spousal bond, and how love is navigated in that relationship.
The father-son bond is central to the boy’s gender self-identity. The father-son bond tends to be less overtly emotional but can be deeply loving, and is vital to the boy’s sense of self-worth and self-esteem. The father-son relationship is the template for the boy’s maturation into being a man.
The mother-daughter relationship is one of the most complex. In this relationship, the maturing daughter role-models her development on her mother, and the mother can sometimes see her own development and vulnerabilities mirrored in her daughter. The mother-daughter relationship also serves as the template for the daughter’s future role behavior as a mother to her own children.
The father-daughter relationship rivals the mother-son relationship for emotional warmth – with daddy’s princess being the classic characterization of this bond. The father-daughter bond is an important source of self-esteem and self-worth for the daughter, and she will use the father-daughter bond as the template for the future spousal bond with her husband.
Each of these relationships is unique. Each is valuable. Each is essential to the child’s healthy development. None of these relationships are expendable.
It is always in the child’s best interest for the family to make a successful transition to a healthy separated family structure.
A cutoff family structure is ALWAYS pathological. There is no such thing as a “healthy cutoff family.”
I want to be extremely clear on this for all of my professional colleagues. There is no such thing as a healthy cutoff family structure. A cutoff family structure is always pathological. Read Bowen. Read the stuff about differentiation of self and emotional cutoffs in the family.
There is no such thing as a healthy cutoff family structure.
It is always in the child’s best interests for the family to make a successful transition to a healthy separated family structure united by the child, and by the child’s bonds of shared affection with both parents.
Divorce ends the marriage, not the family. When there is a child, there is always a family.
Craig Childress, Psy.D.
Clinical Psychologist, PSY 18857
