The pathogen has three defensive structures:
1.) Remain hidden;
2.) Seek allies;
3.) Attack threats of exposure with great viciousness.
I want to talk about the second defensive structure, seek allies. There are several types of allies that the pathogen recruits.
Ignorant Activating Allies: The most obvious allies that the pathogen enlists are the ignorant and incompetent mental health persons who actively collude the pathology because of their profound professional ignorance and incompetence.
The pathogen seeks ignorance, and turns ignorance into an ally. That’s key to remember.
Pathological Activating Allies: In some cases, these mental health allies move from being just plain ignorant and incompetent allies into being pathological allies who are vicariously working through their own childhood trauma histories through their collusion with the false trauma-narrative of the alienation: “abusive parent”/”victimized child”/”protective parent.”
In professional psychology, this is called the therapist’s own “counter-transference” (the patient has “transference” – the therapist has “counter-transference”; transferring childhood patterns to current relationships). These mental health persons have been captivated in their interpretations of the current situation by the “schemas” of their own childhood trauma.
The trauma reenactment narrative of “abusive parent”/”victimized child”/”protective parent” is, psychologically, an incredibly captivating narrative – and it represents the psychological hook that’s used to capture and enlist the ally.
Flying Monkey Allies: Another level of allies are the general “flying monkey” people, these are people like Jean Mercer and the various obsessed general population people who will glom onto a case and escalate the rhetoric with hyperbolic accusations that Gardner, or Childress, or Pruter are evil people seeking to return abused children to their abuser.
This group is similar to the pathological mental health allies in that both groups are working out their own childhood attachment trauma issues by self-adopting the role in the false trauma-reenactment narrative as the “protective ally.” The degree of the inner pathology that’s driving them is evidenced in their obsessional fixation that entirely captivates these flying monkey allies of the pathogen.
The flying monkey allies are typically also the carriers for the pathogen’s third defensive process, attack threats of exposure with great viciousness.
Because the pathogen disables (inhibits) frontal lobe executive function logical reasoning systems of the brain, these flying monkey allies – and all of the pathogen’s allies – are stupid as sin. But the flying monkey allies are also incredibly vicious in their attacks (such as the attack that Gardner was a “pedophile”). They seek to destroy the person. Incredibly vicious.
Because the pathogen is stupid as sin, the attacks emanating from the pathogen aren’t rational. What the attacks lack in rational logic, however, they make up for in sheer number. The attacks emanating from the pathogen are vented a wild barrage of hyperbolic and extreme accusations that are spewed forth in a rapid progression of false allegations, lies, and distortions.
The goal of the pathology is to put the target of the attack on the defensive in order to divert the focus of attention AWAY from the pathogen and thereby relieve the threat of exposure for the pathogen posed by the target. A general rule of thumb for the pathogen is, “When threatened, create complete chaos.”
In addition to putting the target/threat on the defensive, the barrage of accusations is also a strategy to compensate for the pathogen’s inability to logically reason. The pathogen – or more accurately the brain inhabited by the pathogenic structures in the attachment networks – cannot logically reason to be able to figure out what represents rational and reasoned attacks, so instead it throws out a thousand attacks, no matter how irrational, and then follows-up with whatever attacks appeared to gain traction. It’s an interesting strategy for self-defense by a brain in which logical reasoning has been inhibited.
These are the Activating Allies of the pathogen. But there’s a second group of allies, the Enabling Allies of the pathology whose role is to remain hidden beneath the veil of concealment while acting to disable the mental health system’s response to the pathology. As a clinical psychologist, uncovering this aspect of the pathology has been incredibly intriguing, leading to a variety of insights into attachment-related pathology and it’s spread among collateral receptive brain systems.
The Enabling Allies are a trickier group of allies because they operate beneath the pathogen’s veil of concealment – they remain hidden. These allies aren’t as overtly obvious as the Activating Allies, but both groups of allies exhibit the same distinctive inhibition of frontal lobe executive function reasoning systems.
However, the Enabling Allies do not display the same attack motivations as the Activating Allies. Instead, the Enabling Allies exhibit an inhibition of the attack response and a pronounced motivation to seek a stupor of shared-mind states that are marked by a distinctive inhibition of frontal lobe critical thinking. The absence of the attack motivation and the propensity to develop a shared-mind cognitive stupor apparently allows these covert allies to remain hidden and unexposed beneath the pathogen’s veil of concealment, which allows them to then enact their role of deactivating the mental health response to the pathology.
Since the role of these Enabling Allies within the pathology’s social expression is to disable the mental health system’s response to the pathology, putting any solution in place will require that this function of these Enabling Allies of deactivating the mental health system’s response to the pathology must be interrupted, otherwise the pathogen will be successful in continuing to enact itself for another five years or longer, depending on how long the Enabling Allies of the pathogen are able to deactivate the mental health response to the pathology.
Because we will be striving to put into place the solution to “parental alienation” in the coming time period, I need to take steps to interrupt the ability of the pathogen’s Enabling Allies to continue disabling the mental health system’s response to the pathology. To do this, I first need to expose the functioning of these Enabling Allies from beneath their veil of concealment. The first defense of the pathogen is to remain hidden.
Known Pathology
Professional psychology has known exactly what this pathology is for 30 years.
It is abundantly clear to any rational mental health professional that a child’s rejection of a parent is a pathology of the attachment system. The attachment system is the brain system that governs all aspects of love and bonding throughout the lifespan, including grief and loss. A child rejecting a parent is clearly an attachment-related pathology.
That this truth has not been addressed in 30 years by the Gardnerian PAS “experts” represents an appalling absence of professional competence that speaks directly to their absence of motivation to actually solve the pathology.
Are the Gardnerian PAS “experts” really that stupid that they have not recognized in 30 years that a child’s rejection of a parent is fundamentally a pathology of the attachment system? (inhibition of frontal lobe executive function reasoning systems?)
Or are they simply that unmotivated to actually work out and solve the pathology?
Actually, it’s both; the inhibition of frontal lobe reasoning systems and the inhibition of motivation to solve the pathology.
In 1980 – 35 years ago – John Bowlby, the preeminent authority on the attachment system, identified that the “deactivation of attachment behavior” (such as a child rejecting a parent) was the result of “pathological mourning” (the pathological processing of sadness, grief, and loss).
Yet despite this completely available information, nowhere in the literature of Gardnerian PAS over the past 30 years has the linkage to “pathological mourning” ever been identified or examined. This represents an appalling absence of basic professional competence in the assessment and diagnosis of a clearly attachment-related pathology, and it speaks directly to the absence of motivation in the Gardnerian PAS “experts” to actually solve the pathology.
I used to supervise interns and post-doctoral fellows. If a trainee had brought me a case of a child rejecting a parent surrounding divorce, the first thing I would have done is instruct the trainee to read Bowlby’s three volumes on the attachment system, because a child rejecting a parent is clearly – clearly – an attachment-related pathology. But the Gardnerian PAS “experts” never appeared to have done that. In 30 years, they don’t appear to have cared enough to actually try and understand and diagnose the pathology.
That’s just profound professional sloth bordering on professional negligence.
Q: Why were they so incredibly passive in trying to figure out the nature of the pathology?
A: Gardnerian PAS.
These self-appointed “experts” in a supposedly “new form of pathology” were lulled into a professional slumber by the abject simplicity of the Gardnerian PAS model, which supposedly represented a “new form of pathology” that was entirely unique in all of mental health. They didn’t undertake the proper – the proper – professional responsibility of responding to an attachment-related pathology by becoming knowledgeable and competent about the attachment system.
Shame on them. The degree of professional indolence and sloth displayed by the Gardnerian PAS “experts” across 30 years while thousands and thousands of children and families were destroyed represents, in my mind, professional negligence. I would NEVER have accepted such professional indolence and sloth from any mental health intern I supervised, and there is NO excuse from a licensed mental health professional for such indolence and sloth.
A child rejecting a parent is CLEARLY an attachment-related pathology.
The absolutely first thing for ANY mental health professional to do who is assessing, diagnosing, or treating an attachment-related pathology is to read Bowlby’s three volumes on the attachment system. That’s just a basic-basic issue of professional competence.
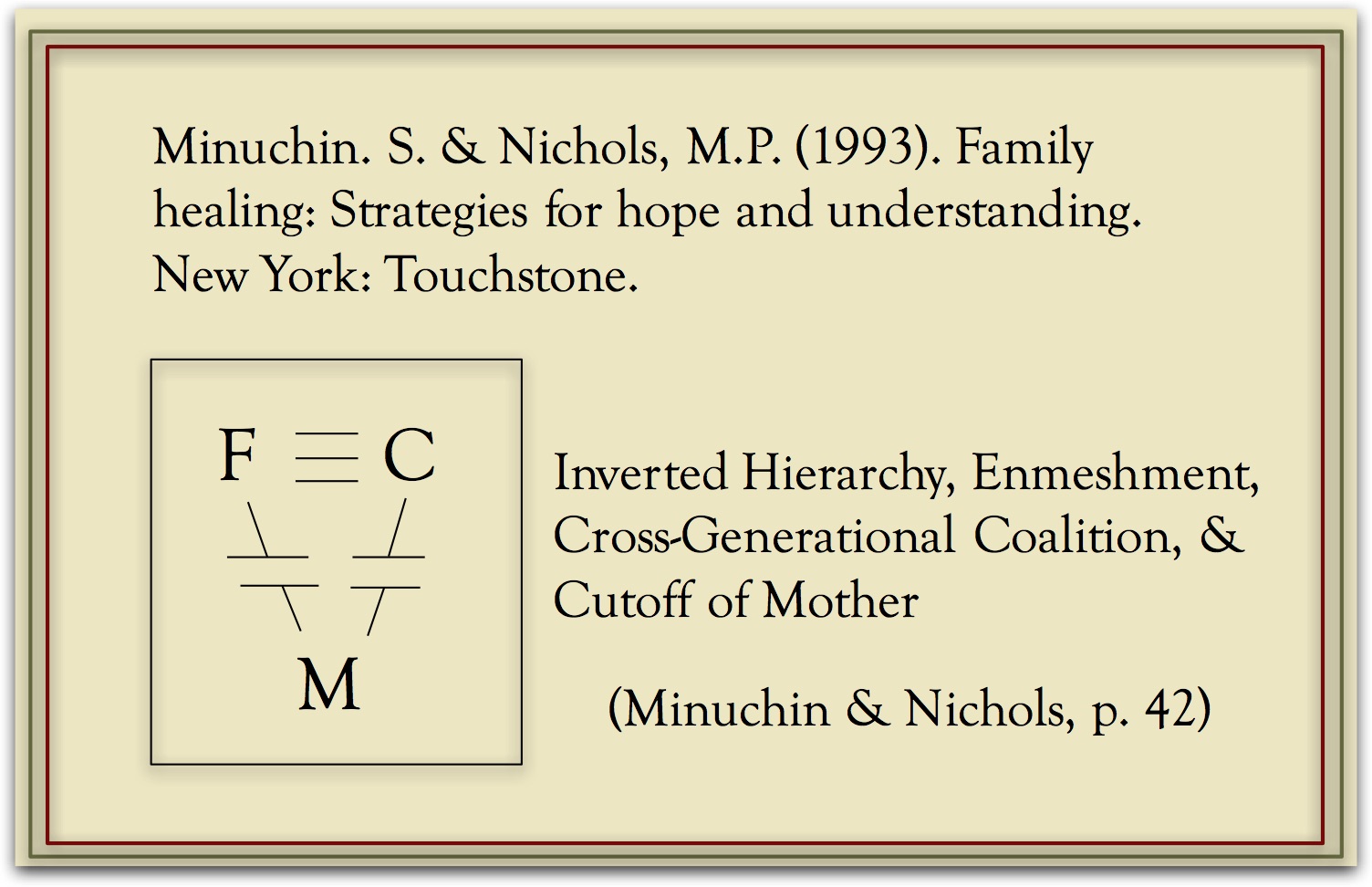
Furthermore, in 1993 – 25 years ago – the renowned family systems therapist, Salvador Minuchin, in his book with Michael Nichols, Family Healing, provided a structural family diagram depicting the pathology that people have been calling  “parental alienation.” This structural family diagram depicts the child’s triangulation into the spousal conflict through the formation of a cross-generational coalition with the father against the mother. Notice the breaks in the lines from the mother to the father and to the child. That’s called an emotional cutoff, and this type of family pathology has been extensively described by the renowned family therapist Murray Bowen (Bowen, 1978; Titelman, 2003).
“parental alienation.” This structural family diagram depicts the child’s triangulation into the spousal conflict through the formation of a cross-generational coalition with the father against the mother. Notice the breaks in the lines from the mother to the father and to the child. That’s called an emotional cutoff, and this type of family pathology has been extensively described by the renowned family therapist Murray Bowen (Bowen, 1978; Titelman, 2003).
That break in the lines depicted in Munichin’s structural family diagram (the “emotional cutoff” in the child’s relationship with the mother) represents the child’s rejection of the parent that everyone is calling “parental alienation.” The correct clinical psychology term for this pathology in family systems therapy is an “emotional cutoff.” Same exact pathology.
Listen to Salvador Minuchin’s description of the consequences of a child’s cross-generational coalition with the mother against the father following the parents’ divorce:
“An inappropriately rigid cross-generational subsystem of mother and son versus father appears, and the boundary around this coalition of mother and son excludes the father.” (Minuchin, 1974, p. 61-62)
“The parents were divorced six months earlier and the father is now living alone… Two of the children who were very attached to their father, now refuse any contact with him. The younger children visit their father but express great unhappiness with the situation.” (Minuchin, 1974, p. 101)
Isn’t that an exact description of the pathology people call “parental alienation” – following the parent’s divorce the children are rejecting one parent (the father in this case) because of a coalition of the children with their mother that “excludes the father.” Look at the date; 1974. Over forty years ago, and fully ten years before Gardner proposed his supposedly “new form of pathology” – his Parental Alienation Syndrome.
This is not some “new form of pathology.” We know exactly what this is. We just need to return to the standard and established constructs and principles of professional psychology.
And then there’s the personality pathology. Gardner identified the “lack of ambivalence” displayed by the child as one of his 8 symptoms of this supposedly new form of pathology. The symptom of a “lack of ambivalence” is called splitting in professional psychology, and is a highly indicative symptom – in fact it’s an exclusive symptom – of narcissistic and borderline personality pathology. Why didn’t Gardner call it splitting? Why didn’t he work out the narcissistic and borderline personality pathology component of the pathology?
This isn’t some sort of “new pathology,” Gardner and the other Gardnerian PAS “experts” are simply poor diagnosticians – in fact, really poor diagnosticians if they have to resort to creating an entirely “new form of pathology.” Let that sink in for a moment. These so-called “experts” are actually horrific diagnosticians, and yet they view themselves as some sort of “experts.” Pretty low bar for “expertise” if you ask me.
Attachment pathology (pathological mourning), family systems pathology (cross-generational coalition and emotional cutoff), personality disorder pathology (narcissistic and borderline personality pathology). Standard and fully established stuff just waiting for us to leave the wilderness of Gardnerian PAS and return to the path of established professional psychology.
Why did this wait 30 years? Not one – not one – of the Gardnerian PAS experts in 30 years put in the professional effort to work this out. Sloth. It’s all been there for the entire time if anyone – if any one of them – had been sufficiently motivated to put in the effort to work it out.
Why did I work it out? Because I am motivated to solve the pathology.
Why didn’t the Gardnerian PAS “experts” work it out? Because they are NOT motivated to solve the pathology.
Simple as that.
But they write articles. They provide testimony. They advocate for PAS to be included in the DSM diagnostic system. Surely they want to solve the pathology?
Writing professional articles as “experts” in a supposedly new form of pathology feeds their inflated narcissistic opinion of themselves as “experts.” Providing “expert” witness testimony feeds their inflated narcissistic opinion of themselves as “experts.” Advocating that PAS be included in the DSM diagnostic system feeds their inflated narcissistic opinion of themselves as “experts.”
They’re not fighting for you. In fact, 30 years – no solution – they are completely impotent in “fighting” for you and your children. And they did not lift a finger to understand and identify the pathology using standard and established constructs and principles that would have provided you and your children with an immediate solution. Why?
Because they don’t want a solution. They want to be “experts.”
They recently had a echo chamber conference in Prague and what did they come up with, all these “experts” in “parental alienation”? That they’re “experts” in “parental alienation.” Seriously. That’s their big news from their conference. Narcissistic self-inflation.
In 30 years they did not do the professional work needed by targeted parents and their children. Why not? Because they don’t actually care about solving the pathology – they just want to satisfy their narcissistic ego-inflation as “experts” in a new form of pathology.
I am waking everyone up to these Enabling Allies of the pathology. We are going to be solving this pathology for all children and all families, and the professional ignorance and incompetence of these Gardnerian PAS “experts” who are actively disabling the mental health system’s response to the pathology needs to stop.
They are false allies to targeted parents and to the children who have endured decades of professional incompetence and professional impotence because of their professional indolence and sloth. They present a fair-face, but they are actually disabling the mental health system’s response to the pathogen. They are false allies to you and your children.
By proposing and supporting a clearly – clearly – inadequate and flawed model of pathology – for 30 years – the Gardnerian PAS “experts” created and continue to create a schism in professional psychology that has disabled the professional response to the pathology in endless and needless debate and internecine professional conflict.
Rather than acting from the proper professional path of describing the attachment-related family pathology using the standard and established – fully available – constructs and principles of professional psychology, these ignorant and incompetent, abhorrently slothful and professionally negligent, Gardnerian PAS “experts” have inflexibly insisted – insisted – that establishment psychology submit to a clearly inadequate and massively flawed model of pathology. And for 30 years, establishment psychology has consistently given them abundantly clear constructive feedback that the Gardnerian PAS model is simply too flawed as a model of pathology.
And it is. It is an absolutely horrific model for a pathology.
Did the Gardnerian PAS “experts” ever take this constructive feedback and set about doing the work necessary to figure out what the attachment-related family pathology of a child rejecting a parent surrounding divorce actually represents? No.
Instead they continued to inflexibly – obstinately – stubbornly – insist that establishment psychology must submit and accept a massively flawed model of pathology. Stupid.
In doing so, they created a vacuum of professional competence. Gardnerian PAS was NOT accepted, but no other model for the pathology was proposed. Into this vacuum of ignorance and incompetence created by the Gardnerian PAS model flowed the massive professional ignorance and incompetence that currently inhabits every corner of the mental health response to the pathology.
The massive professional ignorance and incompetence in the mental health system’s response to this pathology is the DIRECT RESULT of Gardnerian PAS and the professional ignorance, sloth, and incompetence of the Gardnerian PAS “experts.” They are the Enabling Allies of the pathogen. They are the hidden allies of the pathogen who have acted across 30 years to disable the mental health system’s response to the pathology.
How did the pathogen captivate them? By linking into their grandiose narcissistic ego-structures that desire to be regarded as “experts.”
Once the pathogen has them as allies – as Enabling Allies – the pathogen then shuts off their frontal lobe executive function critical thinking systems so they become intellectually slothful and lazy. They like the Gardnerian PAS model because it’s simple. Never mind that its a horrible model of pathology. It’s simple. They can grasp it. It doesn’t make these “experts” think too hard.
And through the motivational networks available from the attachment networks, the pathogen captivates their self-inflated narcissistic motivation to be “experts” while simultaneously inhibiting their motivation to actually solve the pathology. For 30 years they write articles and hold conferences, they advocate and they pontificate – all because they are “experts” in this supposedly new form of pathology. But do they actually solve the pathology. No.
They are not motivated to solve the pathology – they are ONLY motivated to be “experts” in their mythical new form of pathology.
Look what I’ve done with AB-PA. Why? How? Because I am motivated to solve the pathology, not simply be an “expert” in the pathology.
This solution has always – always – been available to the Gardnerian PAS “experts.” From day one. I’m not special; I just care. My motivation is to solve the pathology. Their motivation is to be an “expert.”
Bowlby is not new. 1980. Over 35 years ago.
Minuchin is not new. 1974. Over 40 years ago.
The Gardnerian PAS “experts” have ALWAYS had the ability to solve the pathology – if they had simply wanted to.
They didn’t want to.
Instead, they have locked up the professional response to the pathology in controversy, endless debate, and profound professional ignorance and incompetence – all so they could fulfill their narcissistic self-inflated ego-desires to be “experts.”
Experts. Ha. Stupid as sin.
In terms of actually working to solve the pathology – they have been slothful, intellectually lazy, and entirely impotent in protecting you and your children from the scourge of this horrific pathology – for decades.
The Gardnerian PAS “experts” are the Enabling Allies of the pathogen. They are hiding their ignorance and incompetence behind a false-face of being allies to targeted parents and their children – but they are abandoning – they are sacrificing – targeted parents and their children to the continuation of the pathology, all so that these Gardnerian PAS “experts” can remain narcissistically self-absorbed “experts” in their supposedly new form of pathology.
Their conferences are nothing more that self-congratulatory echo chambers for their own self-aggrandizement, and they will continue to try to lock up the professional response to the pathology in the endless and entirely unnecessary professional “controversy” surrounding their failed, massively flawed, and entirely inadequate model of pathology.
As Enabling Allies of the pathogen, the Gardnerian PAS “experts” will seek to continue to mire professional psychology in a general confusion regarding PAS and AB-PA in order to prevent clarity from emerging that will lead to a solution to “parental alienation.” They will co-opt concepts of AB-PA and associate them with Garnerian PAS even though these concepts are NOT applicable to Gardnerian PAS, all to obfuscate and confuse.
What they seek is to mire the professional discussion surrounding AB-PA in confusion, and because of this AB-PA will be dismissed as simply being Gardnerian PAS and it will take us fully five additional years to undo the damage created by this Gardnerian induced confusion.
All the while, more and more families will be needlessly sacrificed to the pathology, awaiting a solution that is bogged down by the general confusion in professional psychology created by these Gardnerian PAS “experts.”
They have not fought for you. There is no fight in them. But by God, there is fight in me. They are false allies who seek to continue disabling the mental health response to the pathology in order to satisfy their narcissistic self-inflation as “experts” in a mythical form of pathology.
They are now witnessing what “fighting” for targeted parents and their children looks like.
Ignorance from mental health persons will no longer be tolerated. Professional sloth from mental health persons will no longer be tolerated. Professional incompetence from mental health persons will no longer be tolerated. Allies of the pathogen – both Activating Allies and Enabling Allies – will no longer be tolerated.
We will no longer stand by impotently while countless children and their beloved parents are sacrificed to this pathology.
We are going to fight for your children. We are going to bring this pathology to an end.
Craig Childress, Psy.D.
Clinical Psychologist, PSY 18857
Bowlby, J. (1980). Attachment and loss: Vol. 3. Loss: Sadness and depression. NY: Basic Books.
Bowen, M. (1978). Family Therapy in Clinical Practice. New York: Jason Aronson.
Minuchin, S. (1974). Families and Family Therapy. Harvard University Press.
Minuchin. S. & Nichols, M.P. (1993). Family healing: Strategies for hope and understanding. New York: Touchstone.
Titelman, P. (2003). Emotional cutoff in Bowen family systems theory: An Overview. In Emotional cutoff: Bowen family systems theory perspectives, P. Tetelman (ed). New York: Haworth Press.