It became abundantly apparent to me the other day that it’s reached the point that the continuing intransigent ignorance of the Gardnerian PAS “experts” needs to be fully addressed.
The Gardnerian PAS model is in the process of being replaced by the more professional sound and scientifically grounded AB-PA model described in Foundations. These “experts” in Gardnerian PAS will soon become irrelevant because the model they’re holding onto will become irrelevant. We are going to completely solve the pathology of “parental alienation” without reference to the Gardnerian PAS model. Everything is going to be solved.
But it has become apparent to me that the continued propagation of the flawed constructs of Gardnerian PAS actually presents a risk to my kids – (your kids ARE “my kids”) – so I need to take active steps to address and counter the ignorance and professional incompetence surrounding Gardnerian PAS as well.
The professional requirement that ALL mental health professionals be knowledgeable and competent applies to ALL mental health professionals, including the Gardnerians. They too must be knowledgeable in the attachment system, personality disorder pathology, and family systems constructs at a professional level, and they too MUST assess for pathogenic parenting associated with an attachment-based pathology in ALL cases in which attachment-related pathology is evident.
Notice I did not use the term “parental alienation” in any of that statement – we are returning to standard and established constructs and principles of professional psychology to which all mental health professionals – ALL, including the Gardnerians – can be held accountable.
If the Gardnerian “experts” believe themselves to be “exempt” from professional standards of practice regarding professional competence (Standard 2.01a of the APA ethics code) because they are somehow “special” – they’re not.
And if the Gardnerian PAS “experts” think that they are exempt because of their “specialness” from the professional requirements of Standard 9.01a of the APA ethics code regarding their assessment and diagnosis of attachment-related and personality disorder related pathology surrounding divorce – they’re not.
Failure to conduct a proper professional assessment for pathogenic parenting associated with an attachment-related pathology would represent a violation of Standard 9.01a of the APA ethics code for ALL mental health professionals, including the Gardnerian PAS experts.
The statements contained in Slides 43-45 from my Keynote address in Dallas apply equally to the Gardnerian PAS “experts” as they do to every other mental health professional.
Slide 43: Attachment System Competence
Mental health professionals who are assessing, diagnosing, and treating attachment-related pathology need to be professionally knowledgeable and competent in the attachment system, what it is, how it functions, and how it characteristically dysfunctions.
Failure to possess professional-level knowledge regarding the attachment system when assessing, diagnosing, and treating attachment-related pathology would represent practice beyond the boundaries of professional competence in violation of professional standards of practice.
Gardnerian PAS “experts” are not exempt from standards for professional competence in their assessment, diagnosis, and treatment of attachment-related family pathology.
Slide 44: Personality Disorder Competence
Mental health professionals who are assessing, diagnosing, and treating personality disorder related pathology as it is affecting family relationships need to be professionally knowledgeable and competent in personality disorder pathology, what it is, how it functions, and how it characteristically affects family relationships following divorce.
Failure to possess professional-level knowledge regarding personality disorder pathology when assessing, diagnosing, and treating personality disorder related pathology in the family would represent practice beyond the boundaries of professional competence in violation of professional standards of practice.
Gardnerian PAS “experts” are not exempt from standards for professional competence in their assessment, diagnosis, and treatment of personality disorder pathology as expressed within family relationships.
Slide 45: Family Systems Competence
Mental health professionals who are assessing, diagnosing, and treating families need to be professionally knowledgeable and competent in the functioning of family systems and the principles of family systems therapy.
Failure to possess professional-level knowledge regarding the functioning of family systems and the principles of family systems therapy when assessing, diagnosing, and treating family pathology would represent practice beyond the boundaries of professional competence in violation of professional standards of practice.
Gardnerian PAS “experts” are not exempt from standards for professional competence for family systems constructs and principles in the assessment, diagnosis, and treatment of family pathology.
Professional knowledge and competence is required from ALL mental health professionals, including the Gardnerian PAS “experts.”
Gardnerian-Based Ignorance
The need for professional competence from the Gardnerian PAS “experts” became evident to me from a recent website post by Michael Bone, Ph.D., a self-proclaimed “expert” in Gardnerian PAS.
Michael Bone: The Eight Symptoms of PA: Absence of Guilt over Cruelty to and/or Exploitation of the Alienated Parent
I don’t pay much attention to the Gardnerians. Their continued intransigence in holding onto a failed and inadequate model of pathology is simply irrelevant. Gardnerian PAS is going to be replaced by AB-PA. That’s just a fact. So if they choose to hold onto Gardnerian PAS in an effort to remain relevant as “experts” in an outdated and inadequate model of pathology, rather than contribute their professional effort and voices to creating an actual solution to the pathology (AB-PA), then they will ultimately simply recede into irrelevance along with their model of pathology as it’s replaced by the more professionally sound and scientifically grounded model of AB-PA (as described in Foundations).
But I became aware of this article by Dr. Bone when it was linked in a parent support group. The information Dr. Bone presented in this article is deeply troubling because it has the potential to hurt my kids – your kids ARE “my kids.”
The information shared in this article by Dr. Bone was so troubling that I had to respond directly to it in the support group and correct this misinformation propagated by Dr. Bone (who is relying on a Gardnerian model of PAS). Here is my response that I posted in this parent support group:
I generally try not to comment on information shared in support groups as I don’t want to intrude into the discussion. However, in this case I feel obligated to say something to protect the child. This statement is not exactly accurate. The symptom is not an absence of guilt, the symptom is an absence of empathy (a narcissistic trait acquired through the psychological control of the child by a narcissistic/(borderline) parent).
The child actually feels a lot of guilt surrounding having to reject the beloved targeted parent. The child is in a psychological hostage situation. Imagine a wartime hostage who is forced by his or her captors to make derogatory statements about the United States. That soldier feels tremendous guilt about making those statements, even though it was under coercion. That soldier feels like a traitor.
The child of alienation feels tremendous guilt. And in moving forward with the recovery of the child’s healthy love and bonding to the formerly targeted-rejected parent, it is vital for all of the involved adults – therapists and recovered parents alike – to fully understand and provide empathy for the child’s feelings of guilt. We understand. No worries, sweetie. Things got a little out of hand, We can move forward, no worries about it.
In recovering the child, and in providing the child with authentic empathy, we must understand the deep-deep guilt that the child feels for rejecting the beloved targeted parent. Grief and guilt are central to the child’s experience.
The symptom is NOT an absence of guilt. It is an absence of empathy during the active phase of the pathology due to the psychological influence and control of the child by a narcissistic parent who characterologically lacks the capacity for empathy. The child’s symptom of an absence of empathy is coming from the allied narcissistic parent’s absence of empathy.
The authentic child loves the targeted parent, and the authentic child feels tremendous guilt over rejecting the beloved targeted parent. We must be aware of the authentic child in order to provide authentic empathy to the authentic child who is caught in a terrible situation. Empathy heals trauma.
I normally don’t like to intrude, but my client children would want me to clarify this for them. I understand what Gardner was going for with that symptom (i.e., the absence of empathy), but it’s incorrect if we frame it as the absence of guilt.
Craig Childress, Psy.D.
Psychologist, PSY 18857
It was this troubling ignorance from Dr. Bone that made me realize that the time has come to apply standards for professional competence to ALL mental health professionals, including the Gardnerian PAS “experts.” Professional ignorance – and the subsequent incompetence that comes from ignorance – is no longer acceptable… from anyone.
When I read further from this article by Dr. Bone I was also deeply troubled by his apparent absence of professional acumen in his reliance on constructs derived from “mysticism” rather than from professionally established constructs and principles of professional psychology. In his article, Dr. Bone abundantly references the child entering a “trance state” when criticizing the targeted parent. The use of such loose “mystical” terminology by a mental health professional is troubling. Mental health professionals are just that – professionals. We should be describing pathology using the standard and established constructs and principles of the profession. Reliance on constructs derived from “mysticism” – such as “trace states” – is simply unacceptable from a mental health professional.
I understand what Dr. Bone is trying to get at. The proper professional term is a “dissociative state.” Dissociative symptoms are associated with identity disorders, trauma disorders, and are loosely associated with both psychotic disorders and thought disorders. There is a general constellation of pathology in which dissociative symptoms might be evident. Interestingly, dissociative symptoms have also been associated with the psychological decompensation of borderline personality pathology in response to stress:
From: Carlson, E.A., Edgeland, B., and Sroufe, L.A. (2009). A prospective investigation of the development of borderline personality symptoms. Development and Psychopathology, 21, 1311-1334
“Correlational analyses confirmed expected relations between borderline symptoms and contemporary adult disturbance (e.g., self-injurious behavior, dissociative symptoms, drug use, relational violence) as well as maltreatment history.” (p. 1311)
“Trauma and maltreatment undermine the child’s capacity to attend to, recognize, and interpret accurately the cues and affective states of others and by extension, the self. Dissociative processes instill a sense of passivity whereby events are perceived as happening to the individual or controlled outside of the self (i.e., without volition; Breger, 1974; Bowlby, 1969/1982). Children become hypervigilant to the attitudes and intentions of others, further compromising emergent self-awareness, a sense of authorship, and the ability to attend to internal cues, emotional needs, and thoughts.” (p. 1314)
If Dr. Bone, a mental health professional, is going to use “mysticism” terms to describe the child’s symptoms as a “trance state,” then he should at least indicate that he understands the professional pathology he’s describing by referencing the professional terminology of “dissociative state.”
If I wanted to use the construct of a “trance” (and trust me, I wouldn’t) in a sentence to describe the child’s symptom, I might say something like, “In many respects, severely alienated children operate in a kind of trance state (called a dissociative state) where they too may believe the things they are saying, when they are saying them.” This would represent professional practice of indicating that Dr. Bone at least understands the professional construct and it’s associations.
I understand what Dr. Bone is reaching for. The underlying symptom that Dr. Bone is identifying is the encapsulated persecutory delusion of the child (diagnostic indicator 3), and he more directly references this in the second part of his sentence that “they too may believe the [false] things they are saying.”
But Dr. Bone is not applying an AB-PA model. He is trying to fit the child’s pathology into the inadequate Gardnerian PAS model. So he wanders off into “trance states” and absence of guilt rather than remaining professionally grounded in the established professional constructs of dissociative symptoms, encapsulated persecutory delusions, and the absence of empathy associated with narcissistic personality pathology.
It was this display of troubling professional ignorance by Dr. Bone in falsely asserting that these children have an “absence of guilt” and then wandering into the mysticism of “trance states” that made me realize that the time has come to hold ALL mental health professionals accountable to standards for professional competence – even the Gardnerians. The troubling assertion that these children are absent a sense of guilt might lead to efforts to trigger guilt in these children, which would be both cruel and would likely provoke increased rejection symptoms. The use of mystical constructs such as “trance states” rather than a reasoned professional description explaining the presence of dissociative symptoms also further damages our collective professional credibility with establishment psychology (such as with the APA).
Mental health professionals are NOT ALLOWED to be ignorant and incompetent in the assessment, diagnosis, and treatment of your children and families. None of them. Not even the Gardnerian PAS “experts.” It’s time to require professional competence from ALL mental health professionals, even the Gardnerians.
Boundaries of Professional Competence
So I decided to look into this a bit more by examining Dr. Bone’s vitae for evidence of professional competence in the attachment system, personality disorder pathology, and family systems therapy.
Based on my review of Dr. Bone’s vitae, I see no evidence of training or education in the attachment system, personality disorder pathology, or family systems therapy which would be required for professional competence in assessing, diagnosing, and treating attachment-related pathology involving parental personality disorder pathology expressed within family relationships.
Is it any wonder then, that Dr. Bone continues to maintain and propagate a flawed and inadequate Gardnerian PAS model of the pathology, since once the paradigm shifts to AB-PA his “expertise” in Gardnerian PAS will not suffice. Once AB-PA replaces Gardnerian PAS, Dr. Bone will actually need to develop a new expertise in the attachment system, personality disorder pathology, and family systems therapy. It’s much easier, I suppose, to simply hold onto Gardnerian PAS than it is to expend the professional effort needed to obtain true competence in established forms of pathology. With Gardnerian PAS, everyone can just kind of make stuff up without the annoying limitations imposed by having to explain anything using the standard and established constructs and principles of professional psychology.
But the problem is that under the model of professional accountability I described in my Dallas Keynote address, Dr. Bone’s absence of knowledge regarding attachment-related pathology, personality disorder pathology, and family systems constructs would represent a violation of Standard 2.01a of the APA ethics code. Well that’s unfortunate for Dr. Bone. If we establish domains of professional knowledge necessary for professional competence, then he’ll fall into the incompetent area of not knowing what he’s talking about.
I can see why he wouldn’t want AB-PA to become established. But AB-PA offers an immediate solution to the pathology. Quite the dilemma for Dr. Bone. Remain an “expert” or solve “parental alienation.” By his recent post, he’s appeared to have chosen to remain an “expert” in Gardnerian PAS at the sacrifice of a solution to the family pathology of “parental alienation.”
But then, wouldn’t a violation of Standard 2.01a of the APA ethics code make him vulnerable to a licensing board complaint? Yes it would… if Dr. Bone was licensed. But it appears that Dr. Bone isn’t licensed. He apparently surrendered his license in 2007 in order to avoid sanctions. So at this point, as far as I know, Dr. Bone is simply a self-proclaimed “expert” in Gardnerian PAS. And as soon as Gardnerian PAS is replaced by AB-PA, Dr. Bone’s sole “expertise” vanishes.
Curiosity then captured me. What about some of the other prominent Gardnerian PAS “experts,” such as Dr. Bernet, a leading and continuing advocate for Gardnerian PAS? Does he possess the necessary background and training in the attachment system, personality disorder pathology, and family systems therapy necessary to meet professional competence criteria for assessing, diagnosing, and treating attachment-related pathology manifesting through parental personality disorder pathology being expressed in family relationships? So I looked at Dr. Bernet’s vitae for evidence of knowledge, training, and experience in attachment-related pathology, personality disorder pathology, and family systems therapy.
I could find no evidence of a professional level of knowledge or training in the attachment system, personality disorder pathology, or family therapy in Dr. Bernet’s vitae either.
Based on the standards set forth in my Dallas Keynote address that ALL mental health professionals who are assessing, diagnosing, and treating attachment-related and personality disorder pathology that is being expressed within the family need to possess professional-level knowledge of the attachment system, personality disorder pathology, and family systems therapy (Slides 43-45), wouldn’t Dr. Bernet’s seeming absence of professional-level knowledge in these domains mean that he is practicing beyond the boundaries of professional competence in violation of Standard 2.01a of the APA ethics code? Yes it would.
Well that’s unfortunate for Dr. Bernet. So should we just not establish professional standards for knowledge and competence so that Dr. Bernet can continue to be an expert? Or maybe should we provide Dr. Bernet with a “special exception” to the requirement for professional knowledge needed for professional competence? Or should we simply hold ALL mental health professionals accountable to the same standards of practice for professional competence, and ask Dr. Bernet to become knowledgeable about the attachment system, personality disorder pathology, and family systems constructs in order to be considered professionally competent in assessing, diagnosing, and treating this form of attachment-related, personality disorder related, family systems pathology?
But still, wouldn’t the violation of Standard 2.01a of the APA ethics code make Dr. Bernet vulnerable to a licensing board complaint? No. Because Dr. Bernet is an M.D. psychiatrist, not a clinical psychologist, so Dr. Bernet is not subject to the same professional requirements for competence that would bind a clinical psychologist. Whew. Lucky for Dr. Bernet.
What about Amy Baker? So I decided to look at the vitae of Amy Baker. What’s important to note about Amy Baker is that she is not a licensed clinical psychologist. She is a researcher. So she’s never actually assessed, diagnosed, or treated any form of pathology. So her vitae is full of research articles, but no actual experience with assessing, diagnosing, and treating any form of pathology. As I reviewed the titles of her research studies, there are some studies regarding sexualized behavior in children, some studies of children in residential treatment facilities, some studies surrounding Head Start programs. These types of topics are peripherally related to the attachment system. But there is no clear evidence of any studies or professional expertise acquired regarding attachment-related pathology. No reference to insecure attachment types in any of her studies. No indication of the Adult Attachment Interview being used in any of her studies. And there is clearly no indication of any reference to personality disorder pathology or family systems therapy in any of her research.
So if Amy Baker doesn’t have a professional-level of knowledge, training, and expertise in the attachment system, personality disorder pathology, and family systems therapy, wouldn’t that mean she is practicing beyond the boundaries of her competence? No. Because she is not a clinical psychologist who is conducting any sort of assessment, diagnosis, or treatment regarding this form of attachment-related family pathology. She is merely a researcher, and her primary area of research expertise appears to be in trying to document a proposed new form of clinical pathology that is supposedly unique in all of mental health called “parental alienation.”
I will admit that all three of these Gardnerian PAS “experts” are clearly “experts” in Gardnerian PAS. Problem is, there’s actually no such thing in clinical psychology as PAS. I’m a clinical psychologist. I know this sort of stuff. That’s my job. There’s no such thing in clinical psychology as PAS. There’s attention deficit-hyperactivity disorder, there’s autism spectrum pathology, there’s oppositional-defiant and conduct disorder pathology, there are trauma and complex trauma pathologies, there are anxiety disorders, and depressive disorders, and psychotic disorders. There’s all sorts of stuff in clinical psychology. There are even attachment-related pathologies arising from insecure attachments and pathogenic parenting. There’s just nothing about PAS in actual clinical psychology.
Psychological control? Oh yeah, there’s a lot of literature and research about the psychological control of children (see for example, Barber, 2002). There’s stuff about the Dark Triad personality of narcissism, psychopathy, and Machiavellian manipulation, and research that links the Dark Triad personality to revenge in romantic relationships and high-conflict patterns of communication. There’s a lot of research surrounding psychological boundary violations in parent-child relationships and families, including role-reversal relationships in which the child is used to meet the emotional and psychological needs of the parent. All that stuff exists in clinical psychology. Just not PAS.
If we turn to family therapy, there’s the “triangulation” of the child into the spousal conflict through the formation of a “cross-generational coalition” with one parent against the other parent that results in an “emotional cutoff” in family relationships as described by the preeminent family systems therapists Murray Bowen, Jay Haley, and Salvador Minuchin. Family systems therapy is one of the four primary schools of psychotherapy (the others being psychoanalytic, cognitive-behavioral, and humanistic-existential therapy), and family systems therapy is the ONLY school of psychotherapy that addresses the process of resolving current family relationship problems. All the other schools of psychotherapy are individual-oriented models of psychotherapy.
Murray Bowen, Jay Haley, and Salvador Minuchin are among the preeminent figures in family systems therapy, and all of them have addressed, described, and  defined this form of family pathology. In fact, on page 42 of his 1993 book, Family Healing, the preeminent family therapist Salvador Minuchin even provides a structural diagram of the family involving triangulation, a cross-generational coalition, and emotional cutoff.
defined this form of family pathology. In fact, on page 42 of his 1993 book, Family Healing, the preeminent family therapist Salvador Minuchin even provides a structural diagram of the family involving triangulation, a cross-generational coalition, and emotional cutoff.
So there’s all sorts of stuff in actual clinical psychology. There’s just no established and defined pathology of PAS, which is unfortunate for the Gardnerian PAS “experts” because it means that they’re “experts” in a nonexistent form of pathology.
So what happens when we return to standard and established constructs and principles of professional psychology to which ALL mental health professionals can be held accountable? What happens when Gardnerian PAS is replaced by AB-PA? What happens to their status as “experts”? It vanishes. Poof. Once the mythical pathology of “parental alienation” vanishes (notice I’ve always put the term in quotes, from the very beginning of my writing on this topic), so too does their “expertise” because none of these Gardnerian PAS “experts” are expert in actual true forms of attachment-related, personality disorder related, family systems pathologies.
Well, no wonder that none of these Gardnerian PAS experts have come forward to support AB-PA. Why would they support AB-PA if this means they cease to be “experts” in “parental alienation.” I suppose bringing an end to the pathology of “parental alienation” might possibly be a motivation for supporting AB-PA, but obviously not motivation enough.
It’s clear that they want to stop AB-PA from taking hold. They’re trying as hard as they can to simply ignore AB-PA in hopes that it will just go away. I’ve worked in the professional worlds of schizophrenia, and ADHD, and autism, and this is the most interesting thing I’ve ever seen, where a group of professionals act as though significant advancements simply don’t exist. I’m like Lord Voldemort – he who cannot be named. It’s really fascinating to watch.
Allies of the Pathogen
I also find it interesting that there are two groups that want to stop AB-PA. The flying monkey allies of the pathogen, and the Gardnerian PAS experts. Don’t you find that interesting? That these two groups should be on the same side in wanting to stop the solution afforded by AB-PA?
We are reclaiming the citadel of professional psychology for targeted parents and your children. By defining this attachment-related pathology entirely from within standard and established constructs and principles of professional psychology, AB-PA identifies clear domains of professional competence needed for the competent assessment, accurate diagnosis, and effective treatment of this attachment-related, personality disorder family pathology. In defining established domains of knowledge needed for professional competence in the assessment, diagnosis, and treatment of this pathology, AB-PA activates the Standards of the APA ethics code for you and your families, so that you can now hold ALL mental health professionals accountable.
When Gardner led everyone away from the path of professional psychology and into the wilderness of “new forms of pathology,” he allowed the citadel of professional psychology to become infected by the pathogen through its allies, who have effectively disabled the mental health response to this family pathology.
This attachment-related (trauma-related) pathology generates two types allies, the overt “activating ally” and the covert “enabling ally.”
The flying monkey allies of the pathogen are the overt “activating allies” of the pathology who actively collude in the creation of the pathology in order to meet their own (unconscious) psychological needs to be the “protective ally” of the allied narcissistic/(borderline) parent and supposedly “victimized” child.
The Gardnerian PAS “experts” are the covert “enabling allies” of the pathology who (unconsciously) enable the activation of the pathology in order to meet their own (unconscious) psychological needs to play the role of the “protective ally” of the targeted parent and the child. By leaving the path of established professional psychology, the Gardnerian PAS contingent have enabled the profound professional ignorance and incompetence that has effectively disabled the mental health response to this pathology for 30 years.
If the Gardnerian PAS experts are allowed to just make stuff up, then everyone is allowed to just make stuff up, which has led to the rampant and unchecked professional ignorance and incompetence currently surrounding the assessment, diagnosis, and treatment of this attachment-related family pathology. Gardnerian PAS acts to enable the pathogen’s expression by allowing rampant professional ignorance and incompetence that effectively disables the mental health response to this form of attachment-related family pathology.
The supposedly protective “activating ally” of the pathogen who actively colludes with enacting the pathology, and the supposedly protective “enabling ally” who is supposedly the “helpless and ineffectual” ally of the targeted parent and child, are simply flip sides of the same trauma-reenactment coin. Both are meeting their own personal unconscious psychological needs to be the “protective other” in the kabuki theater display of a trauma reenactment narrative.
In order to solve this attachment-related family pathology we must leave the wilderness of “new forms of pathology” and return to the established path of standard and established professional constructs and principles – to which ALL mental health professionals can be held accountable – including the Gardnerian PAS experts. No mental health professional is allowed to just make stuff up. No one.
So Michael Bone, if you want to assert that these children evidence an “absence of guilt,” you’re going to have to explain to me – in detail and at a professional level of analysis – exactly the mechanisms by which the child acquires an “absence of guilt” surrounding the rejection of a parent, because I’m telling you that the symptom displayed by the child is NOT an absence of guilt, it’s an absence of empathy associated with the psychological control of the child (Barber; Kerig) by a narcissistic/(borderline) parent (Beck, Kernberg, Millon) who is the actual source of this symptom display by the child.
I will describe – in detail and at a professional level of analysis; using the standard and established constructs and principles of professional psychology – exactly the mechanisms by which each of the diagnostic indicators and associated clinical signs of AB-PA are created. That’s the standard for professional competence.
So Michael Bone, if you’re going to assert that these children enter a “trance state,” then you’re going to have to explain to me – in detail and at a professional level of analysis – exactly the mechanisms by which this “trance state” is created and triggered. Because I can explain to you – in detail and at a professional level of analysis – exactly how dissociative symptoms emerge from complex trauma, an encapsulated persecutory delusion, and the collapse of parental borderline personality pathology as a result of psychological stress. I can also link these dissociative symptoms to identity pathology in the attachment networks and the trans-generational transmission of trauma.
We are done making stuff up. Done. That applies to ALL mental health professionals, even the Gardnerian PAS “experts.” Bring your “A” game or go away, because these children and families deserve our absolute best. Nothing less is acceptable.
We lead by example. If we expect all mental health professionals to evidence the highest standards for professional knowledge, expertise, and competence, then we must display ourselves the highest standards of professional practice and professional competence. Nothing less than our absolute “A+” game is acceptable.
Domains of Knowledge and Competence
So to Bill Bernet, Amy Baker, Michael Bone and all of the continuing Gardnerian PAS “experts,” you need to identify – specifically – what component of Slides 43-45 from my Dallas Keynote address is wrong.
Because if the statements contained on these Slides are correct, and they are, then you will need to explain why these standards of practice don’t apply to you; why, of all mental health professionals, you are “entitled” to not be competent in the assessment, diagnosis, and treatment of an attachment-related pathology.
If you assert that a child’s rejection of a parent is not an attachment-related pathology, then you will have to explain – in detail and at a professional level of analysis – why a child rejecting a parent is not an attachment-related pathology and you will have to explain – in detail and at a professional level of analysis – why Bowlby’s statement that the “deactivation of attachment behavior” is a key symptom of “pathological mourning” is not true.
Professional competence applies to ALL mental health professionals – Gardnerians included. We lead by example. No mental health professional is exempt from standards of practice for professional competence.
If Gardnerians PAS “experts” are allowed to just make stuff up, then everyone can just make stuff up and we dissolve into rampant and unchecked professional ignorance and incompetence.
The Gardnerian PAS experts are unconsciously acting as covert “enabling allies” of this attachment-related family pathology who are colluding with the disabling of the mental health response to this form of attachment-related family pathology.
All mental health professionals – each and every single one – must now be professionally knowledgeable and competent in the attachment system, personality disorder pathology, and family systems therapy. If you don’t want to bring your absolute “A+” game to the assessment, diagnosis, and treatment of this attachment-related family pathology, then go away, because nothing less than that is acceptable.
We are returning to the path of professional psychology in which all – ALL – mental health professionals will be expected to assess for pathogenic parenting surrounding an attachment-related pathology (using the Diagnostic Checklist for Pathogenic Parenting), including mental health professionals who continue to hold and espouse a Gardnerian PAS model for the pathology. There is no excuse or justifiable reason for ANY mental health professional, including Gardnerian PAS “experts,” not to assess for the three diagnostic indicators of AB-PA pursuant to Standard 9.01a of the APA ethics code for professionally competent assessment.
If you are not going to assess for pathogenic parenting associated with an attachment-related pathology, then you must provide a cogent justification at a professional level of analysis as to WHY you refuse to even assess for pathogenic parenting when assessing attachment-related pathology.
We are leaving the wilderness of “new forms of pathology” and we are returning to the world of professional competence.
If you wish to argue that you are somehow entitled (a narcissistic symptom) to be exempt from the rules that govern all other – “ordinary” – mental health professionals (also a narcissistic symptom) because you alone somehow occupy a special status or elevated position (also a narcissistic symptom), you can try – but it’s not going to work. ALL mental health professionals are accountable to standards of professional practice – including you.
“As a means of demonstrating their power, narcissists may alter boundaries, make unilateral decisions, control others, and determine exceptions to rules that apply to other, ordinary people.” (Beck et al., 2004, 251)
Slides 43-45 of the Dallas Keynote apply to ALL mental health professionals. There are no “exceptions to rules that apply to other, ordinary people” regarding the professional obligation for professional knowledge and competence. I don’t care how important and special you may think you are (grandiosity is a narcissistic symptom), the rules of professional competence apply to you as well.
The statements made in Slides 43-45 of my Dallas Keynote address apply to ALL mental health professionals.
Craig Childress, Psy.D.
Clinical Psychologist, PSY 18857
Dallas Keynote Address
Slide 43: Attachment System Competence
Mental health professionals who are assessing, diagnosing, and treating attachment-related pathology need to be professionally knowledgeable and competent in the attachment system, what it is, how it functions, and how it characteristically dysfunctions.
Failure to possess professional-level knowledge regarding the attachment system when assessing, diagnosing, and treating attachment-related pathology would represent practice beyond the boundaries of professional competence in violation of professional standards of practice.
Slide 44: Personality Disorder Competence
Mental health professionals who are assessing, diagnosing, and treating personality disorder related pathology as it is affecting family relationships need to be professionally knowledgeable and competent in personality disorder pathology, what it is, how it functions, and how it characteristically affects family relationships following divorce.
Failure to possess professional-level knowledge regarding personality disorder pathology when assessing, diagnosing, and treating personality disorder related pathology in the family would represent practice beyond the boundaries of professional competence in violation of professional standards of practice.
Slide 45: Family Systems Competence
Mental health professionals who are assessing, diagnosing, and treating families need to be professionally knowledgeable and competent in the functioning of family systems and the principles of family systems therapy.
Failure to possess professional-level knowledge regarding the functioning of family systems and the principles of family systems therapy when assessing, diagnosing, and treating family pathology would represent practice beyond the boundaries of professional competence in violation of professional standards of practice.

 alienation”) is to create a mental health/legal system partnership that teams an AB-PA Certified mental health professional with an AB-PA Knowledgeable amicus attorney to effectively resolve the attachment-related family pathology of AB-PA (attachment-based “parental alienation”).
alienation”) is to create a mental health/legal system partnership that teams an AB-PA Certified mental health professional with an AB-PA Knowledgeable amicus attorney to effectively resolve the attachment-related family pathology of AB-PA (attachment-based “parental alienation”).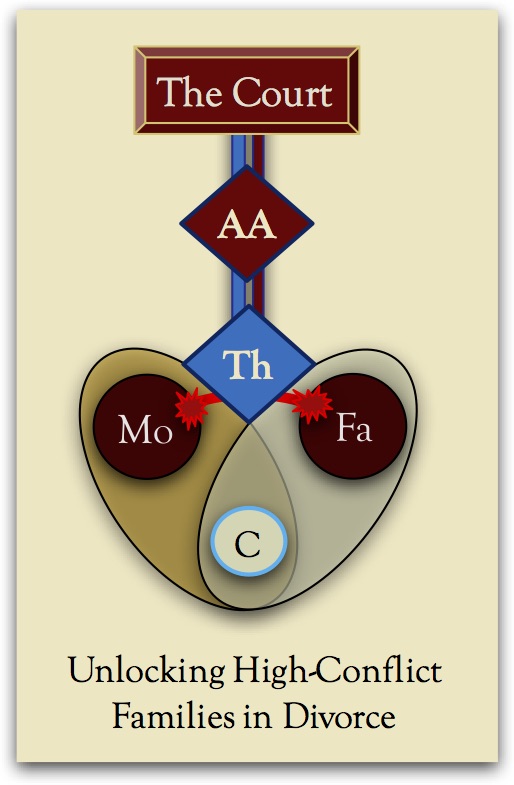 surrounding post-divorce custody and visitation conflict.
surrounding post-divorce custody and visitation conflict.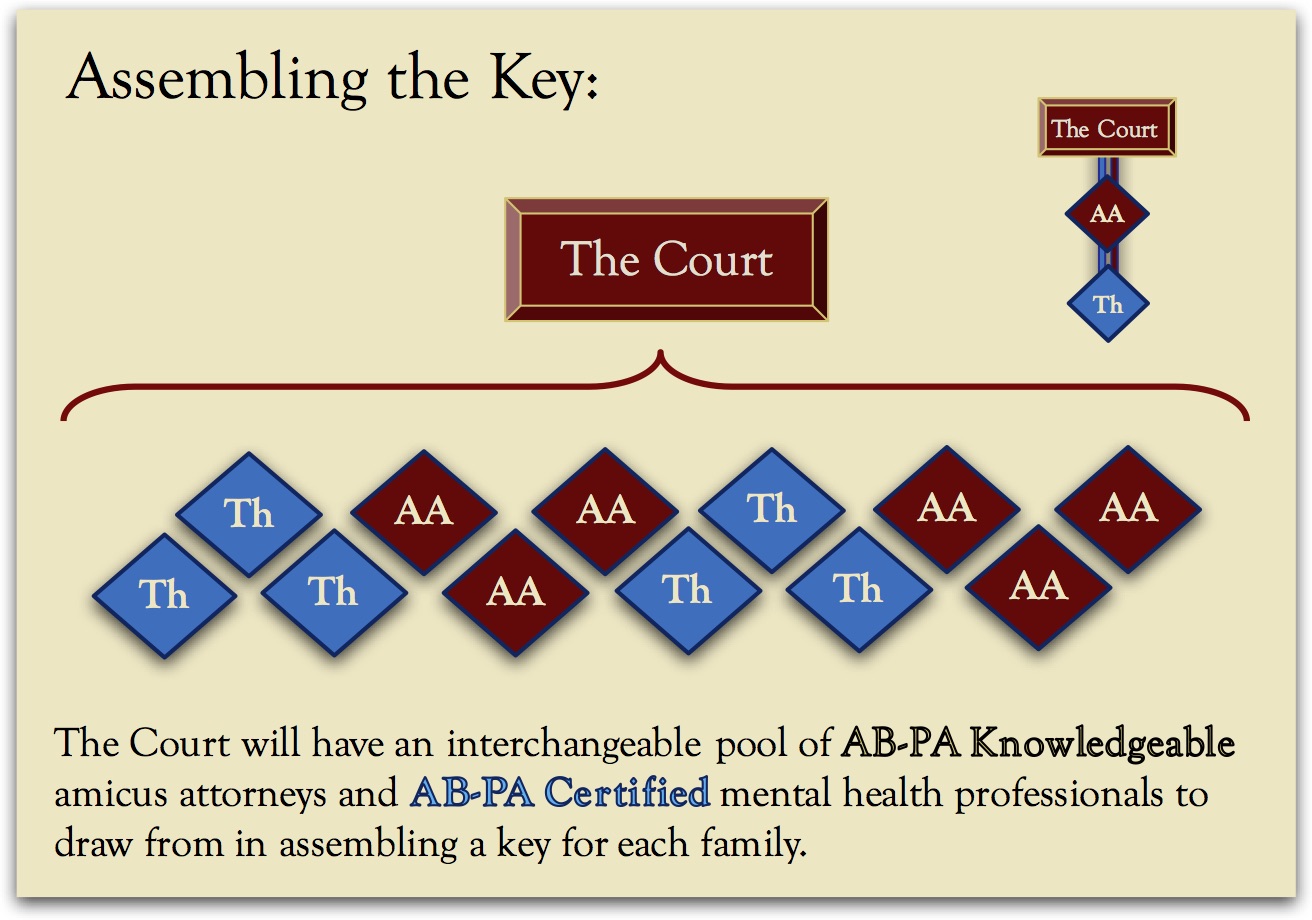 legal expertise needed to assemble an AB-PA treatment Key that teams an AB-PA Certified mental health professional with an AB-PA Knowledgeable amicus attorney.
legal expertise needed to assemble an AB-PA treatment Key that teams an AB-PA Certified mental health professional with an AB-PA Knowledgeable amicus attorney.
