
I have been working with several different attorneys recently who are trying to obtain an appropriate treatment-focused assessment for their clients’ children who are experiencing the attachment-related pathology of AB-PA (the trans-generational transmission of disordered mourning from the allied parent to the child through the formation of a cross-generational coalition of the allied parent with the child against the targeted-rejected parent).
In response to the needs of these attorneys, I have written a formal description of the recommended treatment-focused assessment protocol, and I have been in consultation with the court-involved psychologists regarding the implementation of this assessment protocol.
With the possibility that this recommended treatment-focused assessment protocol may be more broadly helpful to other targeted parents and other attorneys seeking to secure a proper treatment-focused assessment, I have posted this description to my website:
Recommended Treatment-Focused Assessment Protocol
Child Custody or Family Therapy
Divorce is not the end of the family. Divorce is the end of the marriage, but the family continues because of the children.
Divorce simply involves a shift in the family structure from an intact-family structure that is united by the marriage, to 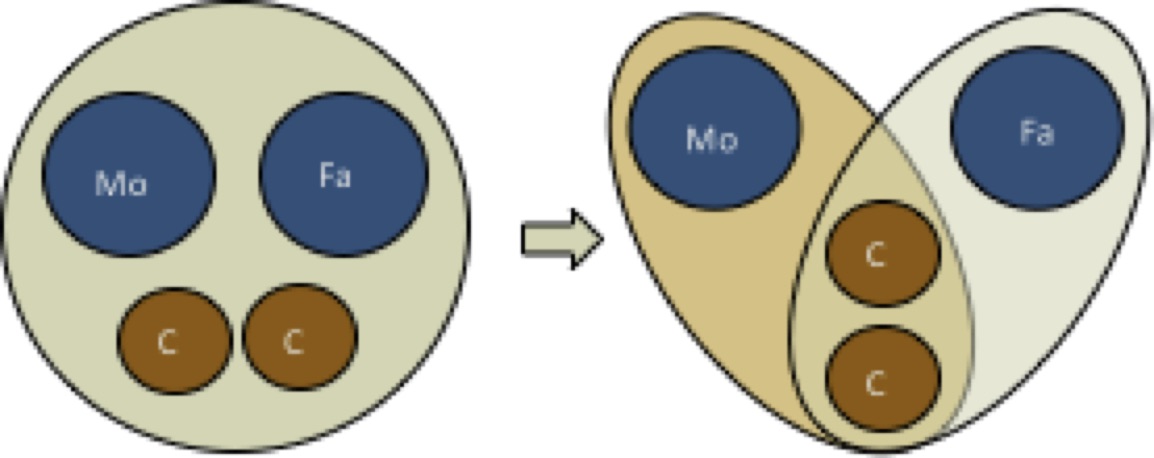 a new separated-family structure that is now united by the children, through continuing co-parenting duties and by the bonds of shared affection between the children and both parents.
a new separated-family structure that is now united by the children, through continuing co-parenting duties and by the bonds of shared affection between the children and both parents.
In high-conflict divorce, the family is having difficulty making this transition from an intact family structure united by the marriage to the new separated family united by the children through the ongoing bonds of shared affection between the children and both parents.
The “splitting” pathology of the narcissistic/(borderline) parent cannot accommodate to ambiguity. In the mind of the narcissistic/(borderline) parent the now ex-spouse must also become an ex-parent as well — the ex-wife must become an ex-mother, the ex-husband must become an ex-father. This is a neurologically imposed imperative of the splitting pathology of the narcissistic/(borderline) parent.
When the splitting pathology of the narcissistic/(borderline) parent is added to the family systems pathology a cross-generational coalition, the already pathological cross-generational coalition is transmuted into a particularly virulent and malignant form that seeks to entirely terminate the other parent’s relationship with the child.
The pathological parenting of the allied narcissistic/(borderline) parent is forcing the child to choose sides in the inter-spousal conflict surrounding the divorce. In the mind of the narcissistic/(borderline) parent, achieving full-custody possession of the child represents a “prize to be won” by whichever parent is deemed to be the “better parent” in their spousal-divorce.
However, the child is not a “prize to be awarded” to the supposedly “better parent” – this is an entirely wrong conceptual framework for understanding child custody.
Children benefit from a complex relationship with both parents. Child custody is not a “competition” between the parents over who is the “better parent” to determine which parent should be awarded the “custody prize” of the child. Children benefit from a complex relationship with both parents.
Except in cases of abusive parenting practices, there is no theoretical or research foundation in professional psychology that would allow us to determine who represents the “better parent.” Parents differ in their approaches. That’s okay. Children love both parents and want the love of both parents in return. That’s normal. Children benefit from a complex relationship with both parents. That’s the reality.
In all cases except child abuse, the recommendation from professional psychology should be for a 50-50% custody time-share. There is no basis in the professional scientific or research literature that would allow professional psychology to differentiate between the potential impact of alternative custody time-share options.
If the parents wish to collaboratively work out a different time-share arrangement, that is their right as parents. But from a professional psychology perspective, there is no theoretical or research foundation that would allow professional psychology to predict the future in any specific situation and determine the relative outcomes from a 60-40% timeshare as compared to a 70-30% timeshare as compared to an 80-20% timeshare as compared a 50-50% timeshare. There are too many exceedingly complex variables.
Except in cases of child abuse, the only professionally responsible recommendation for custody time-share from all mental health professionals is for a 50-50% custody time-share based on the foundational principle that children benefit from a complex relationship with both parents.
A child’s rejection of one parent following divorce and the child’s non-compliance with court orders for custody time-share visitation is a treatment-related issue, not a child custody issue.
Professional psychology should offer the court guidance regarding the treatment needs of the family that are required to help the divorcing family successfully transition from its prior intact-family structure united by the marriage to its new separated-family structure united by the children.
Problems in the family’s transition from an intact-family structure to a separated-family structure following divorce are a treatment-related issue, not a child custody issue.
The allied narcissistic/(borderline) parent is framing the issues as custody-related because of the false belief that the child represents a “prize” in the spousal conflict, to be awarded to whichever spouse is deemed to be the “better parent.”
This false belief in the “child-as-a-prize” to be awarded to the “better parent” is an oft cited argument by the narcissistic/(borderline) parent in these custody disputes; that the other parent “was not an involved parent” prior to the divorce and so should not have equal time-share with the child following the divorce; or that the other parent is not a “good parent” so they don’t “deserve” to have the child in the post-divorce world.
However, the child is NOT a “prize” to be awarded.
Children love both parents and want the love of both parents in return. Children benefit from complex relationships with both parents.
In all cases except child abuse, custody time-share should be awarded 50-50% unless the parents cooperatively agree to a different alternative time-share agreement.
The reason the treatment-related issues within the family become a custody-related conflict is because the narcissistic/(borderline) parent is trying to “win” complete possession of the child (it is a neurologically imposed imperative of the splitting pathology that the ex-spouse must also become an ex-parent; the ex-wife must become an ex-mother, the ex-husband an ex-father).
The child represents a narcissistic prize, a symbol of their victory and superiority, and a weapon to “destroy” the “potential enemy” of the ex-spouse.
“The need to control the idealized objects, to use them in attempts to manipulate and exploit the environment and to “destroy potential enemies,” is linked with inordinate pride in the “possession” of these perfect objects totally dedicated to the patient.” (p. 33)
Kernberg, O.F. (1975). Borderline conditions and pathological narcissism. New York: Aronson.
When professional psychology colludes with this false belief that the role of the assessing mental health professional is to determine the “winner” of the “better parent” competition who will then be awarded the “custody prize” of the child, then professional psychology becomes co-opted into the pathology.
Children love both parents and want to be loved by both parents in return.
Children benefit from a complex relationship with both parents.
Helping the family successfully transition from the prior intact-family structure to the new separated-family structure following divorce is a treatment-related issue, not a child custody issue.
Professional assessments should assist the court in determining the treatment-related needs of the family, not determining the “winner” of the “child custody prize” in the spousal “competition” for the child created by the pathology of the narcissistic/(borderline) parent.
What’s Hard to Understand?
For the life of me, I can’t figure out what’s so hard for mental health professionals to understand about all of this? Granted, the pathology is complex, but its also relatively simple because it is always exactly the same. Understanding psychopathology is what mental health professionals do for a living. It shouldn’t be that hard for them to understand since I have defined the attachment-related pathology in detail across multiple levels of analysis:
Family Systems Level:
At the family systems level, the pathology reflects the inability of the family to transition from an intact-family structure to a separated family structure because of the failure of the narcissistic/(borderline) personality structure to process the grief, loss, and sadness surrounding divorce. The child is being triangulated into the spousal conflict through a cross-generational coalition with the allied-fragile parent against the other parent in order to stabilize the family system in its dysfunctional transition to a new separated family structure.
The attachment-related pathology of a child’s rejection of a normal-range and affectionaly available parent following divorce represents the trans-generational transmission of pathological mourning (Bowlby) from the allied narcissistic/(borderline) parent to the child through the formation of a cross-generational coalition (Haley; Minuchin) with the child against the other parent.
Personality Disorder Level – Splitting:
The addition of parental splitting pathology from a narcissistic/(borderline) parent to the cross-generational coalition with the child transmutes an already pathological cross-generational coalition into a particularly virulent and malignant form that seeks to entirely terminate the child’s relationship with the other parent.
The splitting pathology of the narcissistic/(borderline) personality cannot accommodate to ambiguity. Following divorce, the ex-husband must also become an ex-father; the ex-wife must also become an ex-mother. This is a neurologically imposed imperative of the splitting pathology.
Personality Disorder Level – Projective Displacement of Abandonment-Rejection:
The narcissistic/(borderline) parent is triangulating the child into the spousal conflict as a means to stabilize the collapsing personality structure of the narcissistic/(borderline) parent in response to the inherent rejection and abandonment surrounding divorce. The narcissistic/(borderline) parent is using the child’s induced rejection of the other parent to projectively displace onto the other spouse the core rejection and abandonment fears of the narcissistic/(borderline) parent.
“I’m not the rejected person (spouse) – you are. I’m not the inadequate person (spouse), you are. The child is rejecting you because of your inadequacy as a parent (as a person; (spouse) – you’re the inadequate one, not me. The child is choosing me because I’m the all-wonderful, perfect, and ideal parent (person). The child will never abandon me. You’re the abandoned one; you’re the inadequate and rejected person (spouse), not me.”
Attachment System Level
At its deeper substrate in the attachment networks of the allied narcissistic/(borderline) parent, the pathology represents the trans-generational transmission of attachment trauma from the childhood of the narcissistic/(borderline) parent to the current family relationships, mediated by the personality disorder pathology of the parent that is itself a product of this parent’s childhood attachment trauma.
This trans-generational transmission of attachment trauma is in the schema pattern of “abusive parent”/”victimized child”/”protective parent” that is contained in the internal working models of the narcissistic/(borderline) parent’s attachment networks. It is a false drama – a kabuki theater of display – played out in a false trauma reenactment narrative born in the childhood attachment trauma of the narcissistic/(borderline) parent, a childhood attachment trauma that was responsible for creating the fragile personality structure of the narcissistic/(borderline) parent.
My goodness gracious, how many differing yet interlocking ways, across multiple levels of analysis, do I need to describe the pathology?
Furthermore, I have identified the extensive research literature surrounding the psychological control of the child:
“Psychological control refers to parental behaviors that are intrusive and manipulative of children’s thoughts, feelings, and attachment to parents.” (Barber & Harmon, 2002, p. 15).
The essential impact of psychological control of the child is to violate the self-system of the child.” (Barber & Harmon, 2002, p. 24).
“Rather than telling the child directly what to do or think, as does the behaviorally controlling parent, the psychologically controlling parent uses indirect hints and responds with guilt induction or withdrawal of love if the child refuses to comply. In short, an intrusive parent strives to manipulate the child’s thoughts and feelings in such a way that the child’s psyche will conform to the parent’s wishes.” (Kerig, 2005, p. 12)
“In order to carve out an island of safety and responsivity in an unpredictable, harsh, and depriving parent-child relationship, children of highly maladaptive parents may become precocious caretakers who are adept at reading the cues and meeting the needs of those around them. The ensuing preoccupied attachment with the parent interferes with the child’s development of important ego functions, such as self organization, affect regulation, and emotional object constancy.” (Kerig, 2005, p. 14)
“Parental psychological control is defined as verbal and nonverbal behaviors that intrude on youth’s emotional and psychological autonomy.” (Stone, Buehler, & Barber, 2002, p. 57)
“The central elements of psychological control are intrusion into the child’s psychological world and self-definition and parental attempts to manipulate the child’s thoughts and feelings through invoking guilt, shame, and anxiety. Psychological control is distinguished from behavioral control in that the parent attempts to control, through the use of criticism, dominance, and anxiety or guilt induction, the youth’s thoughts and feelings rather than the youth’s behavior.” (Stone, Buehler, & Barber, 2002, p. 57)
In his book, Intrusive Parenting: How Psychological Control Affects Children and Adolescents, published by the American Psychological Association, Brian Barber and his colleague, Elizabeth Harmon, identify over 30 empirically validated studies documenting the psychological control of children.
I have also identified the research that links the Dark Triad personality comprised of 1) Narcissistic personality traits, 2) Psychopathic personality traits, and 3) Machiavellian manipulation to,
High-Conflict Patterns of Communication:
Horan, S.M., Guinn, T.D., and Banghart, S. (2015). Understanding relationships among the Dark Triad personality profile and romantic partners’ conflict communication. Communication Quarterly, 63, 156-170.
Seeking Revenge in Intimate Relationships:
Giammarco, E.A. and Vernon, P.A. (2014). Vengeance and the Dark Triad: The role of empathy and perspective taking in trait forgivingness. Personality and Individual Differences, 67, 23–29
Rasmussen, K.R. and Boon, S.D. (2014). Romantic revenge and the Dark Triad: A model of impellance and inhibition. Personality and Individual Differences, 56, 51–56
Lying, Manipulative Fabrication, and Deception:
Jonason, P.K., Lyons, M. Baughman, H.M., and Vernon, P.A. (2014). What a tangled web we weave: The Dark Triad traits and deception. Personality and Individual Differences, 70, 117–119
Baughman, H.M., Jonason, P.K., Lyons, M., and Vernon, P.A. (2014). Liar liar pants on fire: Cheater strategies linked to the Dark Triad. Personality and Individual Differences, 71, 35–38
The Absence of Empathy:
Jonason, P. K. and Krause, L. (2013). The emotional deficits associated with the Dark Triad traits: Cognitive empathy, affective empathy, and alexithymia. Personality and Individual Differences, 55, 532–537
Wai, M. and Tiliopoulos, N. (2012). The affective and cognitive empathic nature of the dark triad of personality. Personality and Individual Differences, 52, 794–799
And to Attachment-Related Pathology:
Jonason, P.K., Lyons, M., and Bethell, E. (2014). The making of Darth Vader: Parent–child care and the Dark Triad. Personality and Individual Differences, 67, 30–34
I have developed a simple checklist for the documentation of child symptoms that are created by the pathogenic parenting of a narcissistic/(borderline) parent who is transferring this parent’s own disordered mourning to the child:
The Diagnostic Checklist for Pathogenic Parenting
I have developed a simple rating scale for documenting the normal-range or problematic parenting of the targeted-rejected parent:
Parenting Practices Rating Scale
I have developed a simple relationship rating scale for ongoing treatment-related documentation of the child’s symptoms to facilitate evidence-based documentation and treatment:
Parent-Child Relationship Rating Scale
In Foundations I have elaborated, in great detail, an attachment-based description of the pathology from within each of three distinct levels of analysis, 1) the family systems level, 2) the personality disorder level, and 3) the attachment system level, as well as integrating the description across all three levels, with the attachment system level creating the personality disorder level, and the personality disorder level creating the family systems level. In Foundations, I also describe in detail the distorted relationship-based communication processes by which the child’s rejection of the targeted parent is created.
I have now described a structured Treatment-Focused Assessment Protocol.
Child Protection
At its core, pathogenic parenting is a child protection issue – not a child custody issue.
Pathogenic parenting that is creating significant developmental pathology in the child (diagnostic indicator 1), personality disorder pathology in the child (diagnostic indicator 2), and delusional-psychiatric pathology in the child (diagnostic indicator 3), in order to meet the emotional and psychological needs of the parent represents a DSM-5 diagnosis of V995.51 Child Psychological Abuse, Confirmed.
Assessment leads to diagnosis, diagnosis guides treatment.
Craig Childress, Psy.D.
Clinical Psychologist, PSY 18857
Barber, B. K. (Ed.) (2002). Intrusive parenting: How psychological control affects children and adolescents. Washington, DC: American Psychological Association.
Barber, B. K., & Harmon, E. L. (2002). Violating the self: Parenting psychological control of children and adolescents. In B. K. Barber (Ed.), Intrusive parenting (pp. 15-52). Washington, DC: American Psychological Association.
Kerig, P.K. (2005). Revisiting the construct of boundary dissolution: A multidimensional perspective. Journal of Emotional Abuse, 5, 5-42.
Stone, G., Buehler, C., and Barber, B. K.. (2002) Interparental conflict, parental psychological control, and youth problem behaviors. In B. K. Barber (Ed.), Intrusive parenting: How psychological control affects children and adolescents. Washington, DC.: American Psychological Association.

Reblogged this on Parental Alienation's Dirty Secrets , Akin to Domestic Violence 40 yrs ago.
Happy New Year to you and your family, Dr. Childress Your Treatment-Focused Assessment Protocol is Brilliant
>
Inspired by your recent newsletter (“Arise” 2/1/2017), I will be reaching out to my state senator to discuss the issue of AB-PA and in particular how your Treatment-Related Assessment Protocol can lead to accurate diagnosis and effective treatment. My concern, however, is the presence in the assessment form of the term “parental alienation” (twice), which could run the risk of initiating an automatic and counterproductive response. Is there any chance of replacing those two instances with a less historically-inflamatory term?