
I want to report on a clinical case from my practice, a 16 year-old male adolescent with a significant history of aggression and hostility toward his mother, provoked and supported by his father.
The mental health documentation of the family pathology goes back to 2016. Treatment reports from three prior mental health professionals, two PhD psychologists and an MFT marriage and family therapist, are all in complete agreement. All three diagnosed Child Psychological Abuse in the period from the spring of 2016 to the summer of 2017, with the most recent psychologist giving a formal DSM-5 diagnosis in his written report of V995.51 Child Psychological Abuse (summer of 2017).
Both psychologists, one in 2016 and the other in 2017, expressed concerns about frequent and “inappropriate” kissing on the mouth between the son and father. All three mental health professionals diagnosed the father with extremely pathological narcissistic personality disorder, with strong IPV (Intimate Partner Violence; domestic violence) components of spousal abuse, and directly observed hostile, verbally abusive episodes toward the spouse (and therapist) are reported by multiple therapists.
It took a year and a half from the time that the DSM-5 diagnosis of Child Psychological Abuse was made by the treating psychologist in the summer of 2017 (after the two previous mental health providers also diagnosed psychological abuse) for the mother to finally get a protective separation order from the court. The child was left in the care of a diagnosed abusive parent for 18 months following the formal diagnosis of child abuse by a licensed psychologist with 37 years of professional experience (and after the two prior therapists also diagnosed child abuse by the father).
A year and a half after the DSM-5 diagnosis of Child Psychological Abuse made by the treating psychologist, the court granted the mother’s request for a protective separation order. In February of 2019 the court granted the mother full custody of her snarling, hateful, and aggressively violent 16 year-old son, so that she and her son could receive treatment after years of dominating and controlling, documented psychological abuse of the child by the father had entirely destroyed the child’s relationship with the mother.
Mental Health Reports: Documented Pathology
The first mental health report regarding the family pathology is from the spring of 2016. In it, a psychologist with 40 years of professional experience said,
“The father displayed in my office the most extreme, antagonistic, narcissistic-based behavior I have ever seen.”
“The father’s full manipulation of the child has completely dominated every area of his life, school, friends, family, and in particular, his displays of kissing his father repeatedly on the lips in public, these are all inappropriate. The child lives in constant fear of displeasing his father, and has no independent thinking, apart from what his father requires.”
These are the statements from the report of a PhD psychologist in the spring of 2016.
The next report is from a marriage and family therapist (MFT) who treated the family in the spring and summer of 2017. In this report, the MFT states,
“It is my belief that <child name> is a victim of Child Psychological Abuse from his father. It is my belief that the messages <child name> has been receiving from his father have resulted in significant psychological harm to the child. He is experiencing severe reactions to stress.”
The next mental health report is from a PhD psychologist with 37 years of professional experience. In his report he states,
“It is clear to me that <child name>, who lives with his dad and gets a few hours per week of visitation with his mom, has been mentally and emotionally abused by his father for the past year.”
That was in the summer of 2017. This third psychologist gave a DSM-5 diagnosis of V995.51 Child Psychological Abuse and he referred the child and mother to the High Road workshop of Dorcy Pruter.
In February of 2019, a year and a half after the formal DSM-5 diagnosis of Psychological Child Abuse, a protective separation order was granted by the court and the mother and child entered the High Road workshop.
Following the recovery through the High Road workshop, I became the treating clinical psychologist for follow-up care with the recovered child and restored mother-child bond.
This clinical case report represents the application of a single-case ABA design to assess the effectiveness of the High Road workshop for recovery from complex trauma in childhood. The form of complex trauma is child psychological abuse, created in the context of high-intensity family conflict and parental narcissistic and borderline pathology.
In this current case, the child had been exposed to at least three years of professionally documented child abuse. In February of 2019, the child entered two days – two days – of the High Road workshop. I began treatment of the mother-son relationship following the two days of the High Road workshop conducted by Dorcy Pruter.
During the workshop, Ms. Pruter collected parent rating data every morning and evening for the child’s relationship with the targeted parent, the mother, using the Parent-Child Relationship Rating Scale (PC-RRS). When I began my treatment in March of 2019, I continued to collect the mother’s ratings on the PC-RRS for the child’s relationship behavior with her.
This is a report on the PC-RRS data for a single-case ABA clinical recovery from the complex trauma of psychological child abuse, using the High Road protocol.
Single-Case ABA Research Design
When most people think of research, they think of an experimental research design where many people are separated into different groups, these groups then receive different experimental procedures, and group differences are measured using statistics; the experimental design.
There is a second research methodology that is equally as effective in demonstrating causality, and which is commonly used in assessing treatment efficacy, the single-case research design.
Wikipedia: Single-Subject Design
“In design of experiments, single-subject design or single-case research design is a research design most often used in applied fields of psychology, education, and human behavior in which the subject serves as his/her own control, rather than using another individual/group.”
In a single-case research design, the subject moves through a series of phases of intervention. The initial phase (A) is a baseline assessment phase. This is followed by a period of intervention (B), which is followed by the withdrawal of intervention and return to the baseline of no-intervention (A).
For the single-case ABA clinical recovery and treatment reported here, the initial A (baseline) phase was the pre-intervention (pre-HR) ratings on the Parent-Child Relationship Rating Scale (PC-RRS). The intervention (B) was two days of the High Road workshop conducted by Dorcy Pruter. The withdrawal of intervention (second A) was entry into my clinical care as the treating clinical psychologist following the High Road recovery workshop.
Instrument: PC-RRS
The Parent-Child Relationship Rating Scale (PC-RRS) is a parent rating of three features of the parent-child relationship; Affection, Cooperation, and Social Involvement. During the High Road workshop period, these ratings were made twice daily (morning, evening). In the follow-up clinical care with the treating psychologist, these parent ratings were made daily (end of the day).
The three items rated on the PC-RRS (Affection, Cooperation, and Social Involvement) are rated on a 7-point Likert scale from problematic (1s and 2s) to exceptionally positive (6s and 7s). The Affection scale monitors parent-child attachment bonding. The Cooperation scale monitors emotional disruptions (emotional flexibility and inflexibility). The Social Involvement scale monitors arousal emotions (anxiety, stress, sadness, and depression). The PC-RSS is designed to pick up key features of emotional and psychological functioning in healthy and unhealthy relationships.
The items are structured to reflect a normal-curve distribution, with normal-range being a middle rating of 4, extremely problematic behavior is rated a 1, and highly favorable behavior is rated a 7. The goal for healthy development and for treatment is to achieve reasonably sustained periods of stable normal-range behavior (ratings in the 3 to 5 range) across all three indicators, Affection, Cooperation, and Social Involvement.
Occasional drops into problematic 1 and 2 rated behaviors is normal and is anticipated from time to time in healthy child development. However, sustained periods of low-level ratings of 1s and 2s would indicate issues of clinical concern. Occasional elevations into 6 and 7 behaviors of high affection, cooperation, and social involvement are hoped for and desirable. However, healthy child development is not a sustained period of hyper-affection, hyper-cooperation, and hyper-social involvement.
The goal for child development is a healthy regulated state; mid-range is normal-range. For the most part, healthy child development occurs in a regulated mid-range of flexibility. The treatment goal using the PC-RRS is the mid-range of well-regulated relationship behavior; ratings in the 3 to 5 range for all three scales, Affection, Cooperation, and Social Involvement.
The Data
A: Child Psychological Abuse
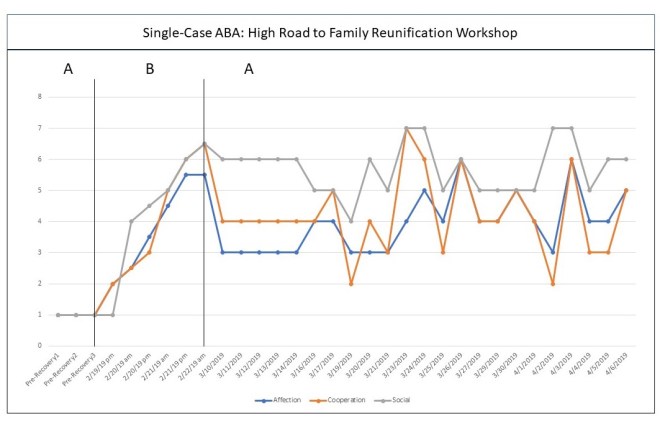
PC-RRS ratings were not collected during the baseline period because the child’s overt hostility toward the mother that was created by the father’s psychological control of the child prevented the mother’s access to the child. The reasonably assigned ratings for the child’s relationship behavior toward the mother during this period, based on reports from three separate clinical therapists, would be Affection=1-2; Cooperation=1-2; Social Involvement=1-2.
B: Intervention – the High Road Protocol
In February of 2019, a protective separation order was granted by the court, and mother and son entered a 2-day High Road workshop conducted by Dorcy Pruter. On their evening arrival the day before the workshop began, the child’s ratings on the PC-RRS were Affection=2; Cooperation=2; Social Involvement=1.
On Day 1 of the workshop, the child’s ratings on the PC-RRS began a rise that would be continual across the 2-day workshop period, reaching an evening rating on the first day of Affection=3; Cooperation=3; Social Involvement 4.5. A normal-range parent-child relationship with the formerly targeted-rejected parent was achieved by the end of the workshop’s first day.
On Day 2 of the workshop, the child’s previous gains continued their improvement, reaching evening ratings at the end of the 2-day workshop of Affection=5.5; Cooperation=6; Social Involvement=6.
The 16 year-old adolescent had gone from a severely problematic relationship with his mother (ratings of 1-2) to a normal-range relationship by the end of the first day (ratings of 3-5), and rose into the highly affectionate, highly cooperative, and highly social range by the end of the second day (ratings of 6-7).
This represents a remarkable recovery of normal-range, and then superior functioning in the parent-child relationship within two days, following three years of documented psychological child abuse by a severely narcissistic personality parent. In one day, the High Road workshop achieved normal-range bonding and normal-range child development. In two days, the High Road workshop achieved superior bonding and healthy child development.
As a clinical psychologist, I am deeply impressed with the documented effectiveness of the High Road recovery workshop for complex trauma in children.
A: Withdrawal of Intervention – Follow-up Care
In March of 2019, I became involved as the follow-up clinical care treatment provider for the mother and son, following the three years of documented child psychological abuse, and two days of the High Road recovery workshop.
My first session with the mother and son begins the first data points for the clinical care ratings. The mother’s initial daily ratings of the parent-child relationship were consistent upon their entry into therapy; Affection=3; Cooperation=4; Social Involvement=6. The recovery gains documented for the High Road workshop are confirmed by the entry data into follow-up care with the clinical psychologist, with five straight data points in the normal-range.
There is no reason to expect that the mother (the formerly targeted-rejected parent) would falsely report a positive relationship that did not exist. If the mother is reporting a normal-range relationship with the child, then this is true and accurate data concerning their relationship. The mother’s daily ratings are discussed in weekly therapy to verify rating calibration and ensure the validity of the ratings. Problematic relationship issues that produce lowered daily scores are discussed in therapy using behavior-chain interviewing to verify rating accuracy and validity.
As therapy began to have impact, the initial stability of the normal-range relationship achieved by the High Road workshop began to fluctuate in response to my treatment interventions. The rise in the ratings surrounding the 3/24/19 period reflects my first session of substantive treatment following my initial entry-sessions. The fluctuations surrounding the 4/3/19 period reflect my second therapy session of substance.
The sensitivity of the PC-RRS ratings to the effects of therapy, with distinctive periods of visible impact from therapy sessions, means that these rating are accurate and sensitive indications of the parent-child relationship. The recovery of healthy and normal-range child development documented during the High Road workshop is confirmed by the treatment data in follow-up therapy.
The High Road workshop recovers children from abuse and trauma, and restores loving bonds of affection and healthy child development. That is a fact. The success of the High Road recovery protocol is documented by evidence, by the data. It is a scientifically established fact.
There’s a reason it’s called a “single-case” research design; causality can be proven in a single case.
Findings of the Single-Case ABA for the High Road Workshop
As the current treating clinical psychologist for the mother and son relationship, it is my confirmed professional opinion that the mother-son affectional attachment bond has been fully recovered by the High Road workshop. Not a doubt in my mind.
The child’s healthy development has been recovered, and the child’s healthy and bonded relationship with his mother has been restored by the High Road workshop of Dorcy Pruter. That is a scientifically confirmed fact. Just look at the data.
From the first moment the mother-son relationship entered my treatment, their relationship was entirely in the normal-range, and their relationship has maintained that stability in response to the intrusions and perturbations introduced by therapy. If the rating scales are picking up the effects of my therapy, the ratings are accurate reflections of the parent-child relationship. Dorcy Pruter achieved a full recovery of the child, in two days… one day actually; normal-range ratings on the PC-RRS were achieved by the end of the first day of the High Road workshop.
The variability in the mother’s scores suggests that she has a sensitive internal calibration for her ratings. The daily ratings are verified in family discussion with the mother and child during the weekly therapy session using behavior-chain interviewing around incidents of concern and ratings. This data is accurate. Not a doubt in my mind.
Following three years of psychological child abuse, child abuse confirmed independently by three separate mental health professionals, Dorcy Pruter and the High Road workshop recovered the child’s healthy and normal-range functioning in two days. That is remarkable.
The success of the child’s recovery is remarkable, the success of Ms. Pruter’s achievement with the High Road protocol is remarkable. Much respect from a licensed clinical psychologist.
The recovery she achieved is verified by the ratings upon entry into my follow-up care, and has remained stable during my treatment period.
Remarkable.
There is a reason it is called a “single-case” design – care to hazard a guess as to why?
The single case research design was the favorite research methodology of B.F. Skinner, a researcher of exemplary talent who helped found the fields of behavioral psychology and learning theory. He didn’t trust the group differences in experimental design that might be “statistically significant” but so small as to be clinically irrelevant. If an intervention is effective, we should be able to see the results. That’s why B.F. Skinner preferred the single-case methodology in his research.
The effectiveness of the High Road workshop is confirmed. I will verify the data points from my therapy, Ms. Pruter will verify her data points from the recovery workshop. It’s true. Absolutely verifiably true. There is documented evidence for the effectiveness of the High Road workshop for recovering children from complex trauma and child abuse.
The High Road workshop represents evidence-based practice.
There’s the evidence. Right there. It’s a lock.
Journal publication will come. The next phase for Ms. Pruter is replication. Do it again.
She has already done it over 100 times. She’s just been so busy recovering children that she hasn’t been focused on research protocols. She has PC-RRS data on many, many families during the workshop. And each new case represents a new single-case ABA. Data will be collected using the PC-RRS for each new workshop and recovery, and the success of recovery – for each case – will be documented by evidence.
The data is in, the High Road workshop is evidence-based practice. There is the evidence, right there, and each new workshop becomes a new single-case ABA, documented using the PC-RRS. Want to replicate this research? Please do.
What my therapy data does, is confirm her data from the workshop. I see the recovery with my own eyes, in my treatment sessions, I see the success of the High Road workshop in the real-world recovery of my client-child and his healthy and bonded relationship with his mom. She is beyond herself with joy.
I’m sure this research will generate further discussion in the months ahead. As far as I’m concerned as a clinical psychologist, it’s a lock. The High Road workshop of Dorcy Pruter is evidence-based practice and it will recover the child’s healthy and normal-range development in a matter of days. That is a scientifically proven fact.
Not a doubt in the world. There’s a reason it’s called a “single-case” design. Just look at the data. How can anyone possibly argue with that. It’s a lock, it’s a fact.
Craig Childress, Psy.D.
Clinical Psychologist, PSY 18857

Cumulative statistical data like this and what Dr. Warshak published in Family Court Review in 2010 is critical so that family courts can be confident ordering the protective separation necessary for psycho-educational interventions. I question “reunification” organizations that don’t have this basic data. Effectiveness must be the standard of care for all practitioners striving to reduce trauma, build resiliency and stop the inter generational transmission of pathology and trauma. I hope that once Dorcy has this effective and efficient protocol established, she will begin to train therapists and advocates all over the country, so that this intervention is available to all struggling families!
To all of my fellow loving parents I found this letter written by a psychologist as what they maybe going through, I found it comforting!
Dear Parent:
This is what I want you to HEAR!
This fight we are in right now. I need it. I need this fight. I can’t tell you this because I don’t have the language for it and it wouldn’t make sense anyway. But I need this fight. Badly. I need to hate you right now and I need you to survive it. I need you to survive my hating you and you hating me. I need this fight even though I hate it too. It doesn’t matter what this fight is even about: curfew, homework, laundry, my messy room, going out, staying in, leaving, not leaving, boyfriend, girlfriend, no friends, bad friends. It doesn’t matter. I need to fight you on it and I need you to fight me back.
I desperately need you to hold the other end of the rope. To hang on tightly while I thrash on the other end—while I find the handholds and footholds in this new world I feel like I am in. I used to know who I was, who you were, who we were. But right now I don’t. Right now I am looking for my edges and I can sometimes only find them when I am pulling on you. When I push everything I used to know to its edge. Then I feel like I exist and for a minute I can breathe. I know you long for the sweeter kid that I was. I know this because I long for that kid too, and some of that longing is what is so painful for me right now.
I need this fight and I need to see that no matter how bad or big my feelings are—they won’t destroy you or me. I need you to love me even at my worst, even when it looks like I don’t love you. I need you to love yourself and me for the both of us right now. I know it sucks to be disliked and labeled the bad guy. I feel the same way on the inside, but I need you to tolerate it and get other grownups to help you. Because I can’t right now. If you want to get all of your grown-up friends together and have a ‘surviving-your-teenager-support-group-rage-fest’ that’s fine with me. Or talk about me behind my back–I don’t care. Just don’t give up on me. Don’t give up on this fight. I need it.
This is the fight that will teach me that my shadow is not bigger than my light. This is the fight that will teach me that bad feelings don’t mean the end of a relationship. This is the fight that will teach me how to listen to myself, even when it might disappoint others.
And this particular fight will end. Like any storm, it will blow over. And I will forget and you will forget. And then it will come back. And I will need you to hang on to the rope again. I will need this over and over for years.
I know there is nothing inherently satisfying in this job for you. I know I will likely never thank you for it or even acknowledge your side of it. In fact I will probably criticize you for all this hard work. It will seem like nothing you do will be enough. And yet, I am relying entirely on your ability to stay in this fight. No matter how much I argue. No matter how much I sulk. No matter how silent I get.
Please hang on to the other end of the rope. And know that you are doing the most important job that anyone could possibly be doing for me right now.
Love, Your Teenager
Reblogged this on Parental Alienation and commented:
A: Child Psychological Abuse
PC-RRS ratings were not collected during the baseline period because the child’s overt hostility toward the mother that was created by the father’s psychological control of the child prevented the mother’s access to the child. The reasonably assigned ratings for the child’s relationship behavior toward the mother during this period, based on reports from three separate clinical therapists, would be Affection=1-2; Cooperation=1-2; Social Involvement=1-2.